DOI: 10.20986/resed.2021.3891/2021
SPECIAL ARTICLE
NEW OPIOIDS WITH DIFFERENT INTRACELLULAR MECHANISM OF ACTION; IS A NEW THERAPEUTIC WINDOW OPENING UP?
NUEVOS OPIOIDES CON DIFERENTE MECANISMO DE ACCIÓN INTRACELULAR; ¿UNA NUEVA VENTANA TERAPÉUTICA SE ABRE ANTE NOSOTROS?
B. Mugabure Bujedo1,2
S. González Santos1
1Departamento de Anestesiología, Cuidados Críticos y Medicina del Dolor. Hospital Universitario de Donostia. San Sebastián, España
2Unidad del dolor, Manejo del dolor agudo y crónico. Hospital Universitario de Donostia. San Sebastián, España
ABSTRACT
Opioids are the most drugs used for the management of acute pain. Conventional opioids are widely used for acute pain management in the postoperative setting. However, a primary concern with conventional opioids is their therapeutic window, the range between doses that produce the desired therapeutic effect (analgesia) and doses that produce unwanted opioid-related adverse events (ORAEs). Conventional μ receptor opioids have a narrow therapeutic window in part because of their mechanism of action (MoA): they bind to μ receptors and non-selectively activate two intracellular signaling pathways, leading to analgesia and to ORAEs. This review explores the clinical potential of μ receptor ligands with differential signaling. Agents with a ’differential signaling” MoA represent an innovative approach that may enhance the therapeutic window. These agents modulate μ receptor activity to selectively engage downstream signaling pathways associated with analgesia while limiting activity in downstream signaling pathways that lead to ORAEs. Meanwhile, differential signaling may fulfill an unmet need in the management of postoperative pain. Oliceridine is a clear exponent of this new opioid generation.
Key words: Opioids, mechanism of action, differential signaling, oliceridine
RESUMEN
Los opioides son los fármacos más utilizados para el tratamiento del dolor agudo. Los opioides convencionales se utilizan ampliamente para el tratamiento del dolor agudo en el entorno postoperatorio. Sin embargo, una de las principales preocupaciones de dichos opioides es su ventana terapéutica, es decir, el intervalo entre las dosis que producen el efecto terapéutico deseado (analgesia) y las dosis que producen efectos adversos relacionados con los opioides (EARO) no deseados. Los opioides convencionales sobre receptores μ tienen una ventana terapéutica estrecha, en parte debido a su mecanismo de acción (MdA): se unen a los receptores μ y activan de forma no selectiva 2 vías de señalización intracelular, lo que provoca analgesia y EARO. Esta revisión explora el potencial clínico de los ligandos de los receptores μ con señalización diferencial. Los agentes con un MdA de "señalización diferencial" representan un enfoque innovador que puede mejorar la ventana terapéutica. Estos agentes modulan la actividad de los receptores μ para activar selectivamente las vías de señalización asociadas a la analgesia, al tiempo que limitan la actividad en las vías de señalización posteriores que conducen a los EARO. Por todo ello, la señalización diferencial puede satisfacer una necesidad no cubierta en el tratamiento del dolor postoperatorio. Oliceridina es un claro exponente de esta nueva generación.
Palabras clave: Opioides, mecanismo de acción, señalización diferencial, oliceridina
Correspondence: Borja Mugabure Bujedo
mugabure@yahoo.es
Received: 18-01-2021
Accepted: 24-10-2021
INTRODUCTION
Conventional opioids, such as morphine, hydromorphone, and fentanyl, are widely used for the treatment of acute pain in the postoperative setting. These μ receptor opioid agonists are effective analgesics for nociceptive pain and are widely used as part of the multimodal approach to acute pain relief, particularly after surgery (1). Many years of opioids research have shown that μ receptors provide the best antinociceptive activity of all opioid receptors, but are also associated with the highest incidence of tolerance, dependence, hyperalgesia and abuse (2). Although vital for analgesic efficacy, agonist activity in the opioid receptor μ is also a source of dose-limiting opioid-related adverse effects (ORAEs) that may include respiratory depression, gastrointestinal effects (e.g., nausea, vomiting, and constipation), effects on the central nervous system (e.g., sedation, dizziness and drowsiness) and pruritus (3,4,5,6). Studies have shown that ORAEs pose a greater risk to patient safety, a longer length of hospital stays, an increase in rehospitalization rates and a higher social health cost (7). In addition, OARs can lead to the limitation of the adequate opioid dose prescribed for the patient, which makes the effectiveness of the analgesics themselves difficult. Inappropriate treatment of postoperative pain in patients demonstrates the need to adjust effective treatment for patients and, in part, demonstrates the need to balance analgesia with opioids and non-opioid drugs, called multimodal analgesia, to improve analgesia and reduce the risk of ORAEs (8,9,10).
The most commonly opioids used for pain treatment act on opioid μ receptor systems. In addition to μ receptors, it has also been shown that kappa and delta opioid receptors activate pain inhibiting pathways in the central nervous system. However, to date, activity mediated by kappa and delta receptors has not shown the rapid, profound and systemic analgesic efficacy of μ opioid agonists such as morphine (11). This review explores recent advances in knowledge of pharmacology, focusing on the development and clinical potential of μ receptor ligands with differential signaling. New opioids with differential signaling-based mechanisms of action, such as oliceridine, open a therapeutic window to explore in the immediate future to improve our care practice.
SEARCH METHODOLOGY
This study deepened the bases of pharmacokinetics to optimize the choice of opioid analgesic. A search of articles published in English during the 20-year period from 2001 to 2021 on the subject was performed in PubMed using the PubMed website of the National Library of Medicine (http://www.ncbi.nlm.nih.gov/PubMed). This search retrieved 586 (on June 21, 2021 at 7:30 pm GMT) articles using a criterion for inclusion of “opioids” & “differential signaling” & “oliceridine” separately and finally in combination and resulted in 112 articles.
After extensive selection, results were reduced to 78 with “oliceridine” as the primary keyword. The researchers analyzed the 78 articles and focused on the most relevant articles, drawing conclusions from these published papers. As a final result, 30 articles were finally included in the literature, focusing on the use of oliceridine. No systematic review or meta-analysis is published and 20 narrative reviews or clinical practice articles were published and only 5 randomized human trials were found (2 in healthy volunteers published in 2014 and 3 controlled trials in the hospital setting of pain treatment published in 2018-2019) (12,13,14) and finally 5 other articles from preclinical studies.
RESULTS AND DISCUSSION
Endpoints of clinical trials on pain management
Only controlled clinical trials of oliceridine were found. It should be noted that much of the available safety data were obtained from preclinical studies, or from clinical studies that assessed adverse effects (AE) as secondary outcomes, with a shortage of prospective studies evaluating the safety profile of oliceridine as its primary outcome. Although several post-hoc analyzes were performed on pooled data from THE APOLLO (12,13) and ATHENA (14) trials, these trials had inherent limitations that may influence the accuracy and generalization of pooled results. For example, APOLLO trials had different pain inclusion criteria (APOLLO-1: numeric rating scale (NRS) ≥ 4 within 9 h after regional anesthesia discontinuation; APOLLO-2 NRS ≥ 5 within 4 h after surgery) used different anesthetic techniques (APOLLO-1: Regional anesthesia; APOLLO-2: General anesthesia), had different treatment periods (APOLLO-1: 48 h; APOLLO-2: 24 h), and were predominantly composed of women (APOLLO-1: 85 %, APOLLO-2: 99 %) and Caucasian (APOLLO-1: 69 %; APOLLO-2: 64 %). The ATHENA trial was an open-ended cohort study without a concurrent control group. Therefore, post-hoc analyzes of these studies are limited by heterogeneity in study design and the influence of possible confounding factors. In addition, antiemetic prophylaxis was suppressed or not standardized in these studies, limiting the conclusions that could be derived with regard to the occurrence of postoperative nausea and vomiting with oliceridine compared with other conventional opioids. Future prospective research should therefore focus on confirming whether oliceridine produces a clinically significant improvement in the risk of developing respiratory depression and gastrointestinal complications compared with conventional opioids.
In addition, the safety and efficacy of oliceridine should be investigated in obstetrical and pediatric populations, as these patients are considered to be at increased risk for ORAEs. The role of oliceridine should also be delineated in the context of enhanced recovery after surgery protocols, especially because the use of multimodal analgesia to reduce opioid use and ORAEs is a key principle of enhanced recovery after surgery. Currently, however, the use of oliceridine with multimodal analgesia was only evaluated in the ATHENA (14)trial, and more data are needed to ensure the safety and efficacy of oliceridine when used in conjunction with other analgesics such as paracetamol and non-steroidal anti-inflammatory drugs.
An important pharmacological limitation of conventional opioids is the therapeutic window, i.e., the range between the dosage producing the analgesic therapeutic effect and the dosage at which they cause unwanted AE. Therefore, in clinical practice, the dosage of these drugs may be restricted due to their side effect profiles leading to poorly controlled pain. Notably, this therapeutic window is especially narrow for certain risk populations including patients with chronic obstructive pulmonary disease, renal failure, obesity, sleep apnea, elderly and pediatric patients (6,7,8).
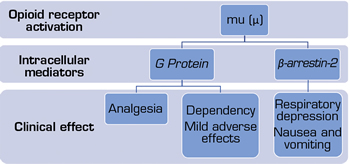
Conventional opioids bind predominantly to μ receptors and unselectively activate 2 intracellular signaling pathways. This binding results in the activation of inhibitory G-protein and β-arrestin-2 pathways, leading to both expected and unwanted pharmacological effects. Activation of G-protein-mediated analgesia and other mid-level effects at the central level, while recruitment of β-arrestin-2 has been shown to contribute to respiratory depression and effects on the gastrointestinal system, and inhibition of G-protein-mediated analgesia feedback (15,16) (Figure 1). Agents with a “differential signaling “ mechanism of action represent a novel and innovative approach. This involves selective activation of specific pathways, i.e., modulation of receptor μ activity to selectively activate intracellular pathways associated with analgesia, while limiting downward activation of signal transduction pathways leading to AE. Recent studies have led to the discovery of new molecules that take advantage of differential signaling in the μ receptor in the hope of improving the therapeutic window. These include oliceridine (TRV 130), PZM21, mitragynine pseudoindoxyl, TRV0109101 and SR-17018 (17,18,19).
Fig. 1. Activation of the mu (μ) opioid receptor and intracellular pathways of both analgesia and adverse effects (15,16).
Conventional opioid receptor signaling
The μ-opioid receptor (a G-protein-coupled receptor) is the primary target of opioid analgesics. Agonists bind to the μ receptor and stabilize conformations that activate heterotrimeric G proteins, leading to signaling of the second messenger (e.g., cycladenosine monophosphate and activation of multiple downstream pathways, including those that lead to pain modulation. Activated receptors are also substrates for G-protein-coupled receptor kinases. After phosphorylation, the receptors bind to the β-arrestin-2, which promotes different downstream effects (20). This process effectively decouples the receptor and G proteins (thus preventing further signaling), promotes the internalization of the receptor and induces different signal transduction cascades. Conventional opioids bind to specific receptors and are not selective in their downstream intracellular signaling after binding. Binding of opioids results in activation of both protein G and the β-arrestin-2 pathway, resulting in both desired and unwanted pharmacological effects. G-protein signaling modulates analgesia, while β-arrestin-2 recruitment contributes to respiratory depression and opioid-induced gastrointestinal effects, and feedback inhibition of G-protein-mediated analgesia. For example, mice lacking β-arrestin-2 have a marked attenuation of respiratory suppression and acute constipation induced by morphine (21). In contrast, morphine-induced analgesia was enhanced and prolonged in these mice, including slower development of tolerance (22). Therefore, a different downstream signaling involving activation of G-protein signaling while limiting β-arrestin-2 recruitment has the potential to expand the therapeutic window of opioids with respect to major respiratory and gastrointestinal improvements (23).
Differential signaling
Given the downward signaling profile of conventional opioids, agonists that are specific to the μ receptor but show preferential differential signaling to G-protein signaling with reduced or even inhibitory effects on β-arrestin-2 signaling have an important potential clinical utility (15,16). Differential signaling in the μ receptor represents a novel and innovative approach to the treatment of postoperative pain, with the opportunity to modulate the activity of the μ receptor to selectively activate the descending intracellular pathways associated with analgesia (protein G) versus those associated with the AE (β-arrestin-2). Several approaches have been adopted to identify μ receptor ligands showing selective signaling, including structure-based ligands, natural product derivatives, and empirical medicinal chemistry (17,18,19). Several of these compounds are believed to have direct clinical potential or will pave the way for other candidate drugs. Their development will improve our knowledge and understanding of receptor μ pharmacology, including the therapeutic window associated with differential signaling in receptor μ polymorphisms, because the large interpersonal variability in the genetic expression of the various opioid receptors has been demonstrated in healthy volunteers (24). Oliceridine is the highest exponent of this group.
Oliceridine
Among the differential signaling ligands being developed, only oliceridine has reached clinical studies. Published phase 1 and 2 studies on oliceridine have shown that its therapeutic window is wider compared with morphine. Oliceridine has a binding efficacy of protein G comparable to that of morphine, but only about 14 % of recruitment via β-arrestin-2, and in relation to the latter, oliceridine also exhibits minimal internalization of receptors (25). In studies in healthy volunteers, oliceridine demonstrated analgesic efficacy, but caused less gastrointestinal dysfunction and respiratory depression than morphine in equianalgesic doses (26,27) Oliceridine has not yet been investigated in a patient population for more than 48 h, but results in postoperative phase 3 pain are promising (12,13,14) and has been approved by the U.S. Food and Drug Administration (FDA) in August 2020 for the intravenous management of severe acute pain (28).
Specifically, in a clinical trial of postoperative pain after abdominoplasty (13), patients received a loading dose of placebo, oliceridine (1.5 mg) or morphine (4 mg), followed by demand doses using patient-controlled analgesia (0.1, 0.35, or 0.5 mg oliceridine;1 mg morphine or placebo) with a blocking interval of 6 min. The primary endpoint was the proportion of people who responded to treatment for more than 24 h for oliceridine regimens compared with placebo. Secondary objectives included a predefined composite measure such as the respiratory safety index (RSI), which represents the cumulative duration of respiratory depression events) and the proportion of responders compared with morphine. A total of 401 patients were treated with study medication. Effective analgesia was found for all oliceridine regimens, with response rates of 61.0, 76.3 and 70.0 % for regimens of 0.1, 0.35 and 0.5 mg, respectively, compared with 45.7 % for placebo (all p < 0.05) and 78.3 % for morphine. The demand dose regimens of 0.35 and 0.5 mg of oliceridine were the same as analgesics as morphine using a non-inferiority analysis. The RSI showed a dose-dependent increase in oliceridine regimens (mean hours [standard deviation], 0.1 mg: 0.43 [1.56]; 0.35 mg: 1.48 [3.83]; 0.5 mg: 1.59 [4.13]; all comparisons are not significant at p > 0.05 vs. placebo: 0.60 [2.82]). The RSI measure for morphine was 1.72 (3.86) (p < 0.05 vs. placebo). Gastrointestinal adverse events increased dose-dependent in oliceridine demand dose regimens (0.1 mg: 49.4 %; 0.35 mg: 65.8 %; 0.5 mg: 78.8 %; vs. placebo: 47.0 %; and morphine: 79.3 %). Compared with morphine, the proportion of patients experiencing nausea or vomiting was lower with the 2 oliceridine equianalgesic dose regimens of 0.35 and 0.5 mg. Safety comparisons with morphine are only relevant for the 2 groups of 0.35 and 0.5 mg equianalgesic doses because the low-dose regimen of oliceridine 0.1 mg was higher than placebo but not as effective as the morphine regimen. These two dose regimens showed a favorable safety and tolerability profile for respiratory and gastrointestinal AE. These findings support that oliceridine may provide a new treatment option for patients with moderate to severe acute pain where intravenous opioid use is warranted.
The objective of another open-label, multicenter phase 3 study was to assess the safety and tolerability of intravenous oliceridine for moderate to severe acute pain in a large population of real-world patients, including postoperative surgical patients and non-surgical patients with painful medical conditions (14). Adult patients with a NRS score for analgesia of ≥ 4 out of 11 pain intensity points received intravenous oliceridine in bolus or patient-controlled analgesia and multimodal analgesia was permitted. Safety was assessed using AE reports, study interruptions, clinical laboratory, and vital signs measurements. A total of 768 patients received oliceridine. The mean age was 54.1 years, with 32 % ≥ 65 years old. Most patients were women (65 %) and Caucasians (78 %). Surgical patients constituted the majority of the study population (94 %), with orthopedic procedures (30 %), colorectal procedures (15 %) or gynecologic procedures (15 %) being the most common. Multimodal analgesia was administered to 84 % of the patients. Oliceridine provided a rapid reduction in the NRS pain score by 2.2 ± 2.3 at 30 min from a score of 6.3 ± 2.1 (at baseline) that was maintained until the end of treatment. No significant cardiorespiratory events or deaths were reported. The incidence of AE leading to early discontinuation and severe AE was 2 % and 3 %, respectively. The most frequent AE were nausea (31 %), constipation (11 %) and vomiting (10 %). Most of the AEs were of mild (37 %) or moderate (25 %) severity and were considered possible or likely to be related to oliceridine in 33 % of patients. The final conclusion was that intravenous oliceridine for the treatment of moderate to severe acute pain was generally safe and well tolerated in the patients studied.
Regarding morphine, another team analyzed previous results in healthy volunteers (29). Data from a previous trial comparing respiratory and analgesic effects of oliceridine and morphine in healthy male volunteers were re-analyzed (n = 30). A population-based pharmacokinetic-pharmacodynamic analysis was performed that served as a basis for the construction of useful functions, which are objective functions of the probability of analgesia, P(analgesia), and the probability of respiratory depression, P(respiratory depression). The utility function = P(analgesia ≥ 0.5)-P(respiratory depression ≥ 0.25), where analgesia ≥ 0.5 is the increase in the latency of hand withdrawal in the cold pressor test by at least 50 %, and respiratory depression ≥ 0.25 is the decrease in hypercapnic ventilatory response by at least 25 %. The values recorded were the median ± the standard error of the estimate. Both drugs were equianalgesic with similar potency values (oliceridine: 27.9 ± 4.9 ng/ml; morphine 34.3 ± 9.7 ng/ml; power ratio, 0.81; 95 % CI: 0.39-1.56). A 50 % reduction in hypercapnic ventilatory response caused by morphine occurred at an effect-site concentration of 33.7 ± 4.8 ng/mL, while a 25 % reduction caused by oliceridine occurred at 27.4 ± 3.5 ng/ml (power ratio, 2.48; 95 % CI:1.65-3.72; p < 0.01). In the clinically relevant concentration range of 0-35 ng/ml, the useful function of oliceridine was positive, indicating that the probability of analgesia exceeds the probability of respiratory depression. In contrast, morphine function was negative, which reveals a larger likelihood of respiratory depression than analgesia. These data indicate a favorable oliceridine safety profile compared to morphine when considering analgesia and respiratory depression in the clinical concentration range.
Therefore, oliceridine is a μ-receptor G-protein pathway selective (μ-GPS) modulator with differential receptor signaling compared to conventional opioids and the only example of this approach in active clinical development for pain. Clinical studies have shown that oliceridine offers rapid improvement and clinically significant pain relief in the acute postoperative period. In equianalgesic doses with morphine, oliceridine showed a better profile of side effects with a lower prevalence of respiratory depression, nausea and vomiting than morphine; thus, thanks to its ability to limit the recruitment of β-arrestin-2, oliceridine can demonstrate a broader therapeutic window. In the context of a multimodal approach, the ability of oliceridine to expand the therapeutic window can lead to significant progress in the treatment of acute pain, enhancing the analgesic the efficacy of opioids, while substantially reducing AE (30).
CONCLUSIONS
Conventional opioid therapies are not selective in their intracellular signaling after binding to μ receptors, activating both protein G and β-arrestin-2 signaling. This signaling profile is associated with analgesia; however, it also results in dose-limiting gastrointestinal and respiratory AE. Therefore, a key unmet need in the treatment of acute pain has been the development of new therapies with a broader therapeutic window than conventional opioids. Differential modulation of μ receptor signaling pathways represents a novel approach to addressing this unmet need in the treatment of moderate to severe acute postoperative pain.
Oliceridine is a μ-protein G modulator with differential signaling at the receptor compared to conventional opioids and the only example of this approach in active clinical development for pain. Clinical studies have shown that oliceridine offers rapid and clinically significant pain relief in the acute postoperative setting. At equianalgesic doses with morphine, oliceridine showed a better profile of side effects, with a lower prevalence of respiratory depression, nausea and vomiting than morphine; therefore, thanks to its ability to limit the recruitment of β-arrestin, oliceridine can demonstrate a broader therapeutic window. In the context of a multimodal approach, the ability to expand the therapeutic window can lead to significant progress in the treatment of acute pain, enhancing the analgesic efficacy of opioids and, at the same time, substantially improving the efficacy of morphine while reducing AE.
The analgesic efficacy of oliceridine was established in several clinical studies, and is FDA-approved for the treatment of moderate to severe acute pain. However, more prospective studies are needed to compare their AE profile with conventional opioids and to assess the cost-effectiveness of their use. In addition, it should be tested for use in obstetric and pediatric populations and in the context of enhanced recovery after surgery protocols.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES