
DOI: 10.20986/resed.2022.3885/2021
ORIGINAL
PRELIMINARY STUDY ON THE EVALUATION OF MECHANICAL PRESSURE PAIN AND CENTRAL PAIN MODULATION MECHANISMS BY ALGOMETRY IN AN ANESTHESIA UNIT
ESTUDIO PRELIMINAR SOBRE LA EVALUACIÓN DEL DOLOR MECÁNICO A LA PRESIÓN Y LOS MECANISMOS DE MODULACIÓN CENTRAL DEL DOLOR MEDIANTE ALGOMETRÍA EN UNA UNIDAD DE ANESTESIA
S. Ayala Pastorino1
G. Varaldi Azcoytia1
L. Illescas Calegari1
P. Castromán Espasandín1
1Departamento y Cátedra de Anestesiología. Hospital de Clínicas. Facultad de Medicina. Universidad de la República. Montevideo, Uruguay
ABSTRACT
Introduction: Pressure algometry is a valid method to evaluate the sensory system of pain transmission in humans, using tests such as temporal summation and conditioned modulation of pain. The objective of this work was to carry out a preliminary experience in the Anesthesiology Service of our University Hospital, using pressure algometry as a quantitative sensory test.
Methodology: In a first stage, a cross-sectional case-control study was carried out, without randomization, where the pressure pain threshold was measured by pressure algometry in 58 patients who consulted in the preoperative evaluation visit. Eighteen had some type of chronic pain (pain group) and 40 had no pain (pain-free group). In a second stage, an observational study was carried out on 36 healthy volunteers, anesthesiology residents. Temporal summation was studied in 16 and conditioned modulation of pain in 20, in both cases using pressure algometry. The application of cuff pressure to the arm was used as a heterotopic stimulus. Both tests were measured at the level of the right trapezius muscle.
Results: In the group with pain, the pressure pain threshold value was lower than in the group without pain in all the points evaluated. The pain threshold value at the mean pressure of the four regions analyzed in the group with pain, turned out to be lower than in the group without pain, 32.7 ± 10 Newtons versus 42 ± 11.7 Newtons (p = 0.004). The mean pressure pain threshold was lower in female patients than in male patients, 36.6 ± 9 Newtons versus 48 ± 11 Newtons (p = 0.001). In the 20 healthy volunteers who underwent the conditioned modulation of pain test at the trapezius level, the pain threshold at the initial pressure was 63 ± 27 Newtons and the final pressure was 72 ± 28 Newtons, with an average increase of 9 Newtons (14.2 %). In the 16 in which the temporal summation test was carried out, it was found that the pain level of the numerical visual scale went from 4.1 ± 1.0 to 6.5 ± 1.5 between the first and tenth stimulus.
Conclusions: The application of pressure algometry in patients who consulted in the preoperative polyclinic, showed that pain thresholds at mean pressure were lower in female patients with chronic pain. In healthy volunteers, temporal summation showed an increase in pain intensity as a normal expression of the "wind-up" phenomenon. In 80 % of healthy volunteers, conditioned pain modulation resulted in an increase in pressure pain threshold with the application of a heterotopic pain stimulus. Pressure algometry is a useful and practical instrument. The information obtained with the quantitative sensory tests can be very useful in the Acute and Chronic Pain Units.
Key words: Quantitative sensory test, pressure algometry, temporal summation, wind-up, conditioned modulation of pain
RESUMEN
Introducción: La algometría de presión es un método válido para evaluar el sistema sensorial de transmisión del dolor en seres humanos, mediante pruebas como la sumación temporal y la modulación condicionada del dolor. El objetivo de este trabajo fue la realización de una experiencia preliminar en el Servicio de Anestesiología de nuestro Hospital Universitario, utilizando la algometría de presión como test sensorial cuantitativo.
Metodología: En una primera etapa, se realizó un estudio transversal de caso y control, sin aleatorización, donde se midió el umbral de dolor a la presión por algometría de presión a 58 pacientes que consultaron en la policlínica preoperatoria. Dieciocho tenían algún tipo de dolor crónico (grupo con dolor) y 40 no tenían dolor (grupo sin dolor). En una segunda etapa, se realizó un estudio observacional a 36 voluntarios sanos, residentes de anestesiología. En 16 se estudió la sumación temporal y en 20 la modulación condicionada del dolor, en ambos casos utilizando la algometría de presión. La aplicación de presión con manguito en el brazo se utilizó como estímulo heterotópico. Ambas pruebas fueron medidas a nivel del músculo trapecio derecho.
Resultados: En el grupo con dolor el valor del umbral de dolor a la presión fue menor que en el grupo sin dolor en todos los puntos evaluados. El valor del umbral de dolor a la presión promedio de las cuatro regiones analizadas en el grupo con dolor, resultó ser menor que en el grupo sin dolor, 32,7 ± 10 Newtons versus 42 ± 11,7 Newtons (p = 0,004). El umbral de dolor a la presión promedio resultó más bajo en pacientes de sexo femenino que en los de sexo masculino, 36,6 ± 9 Newtons versus 48 ± 11 Newtons (p = 0,001). En los 20 voluntarios sanos en los que se realizó la prueba de modulación condicionada del dolor a nivel del trapecio, el umbral de dolor a la presión inicial fue de 63 ± 27 Newtons y el final fue de 72 ± 28 Newtons, con un aumento promedio de 9 Newtons (14,2 %). En los 16 en los que se realizó la prueba de sumación temporal se encontró que el nivel de dolor de la Escala Visual Numérica pasó de 4,1 ± 1,0 a 6,5 ± 1,5 entre el primer y décimo estímulo.
Conclusiones: La aplicación de la algometría de presión en pacientes que consultaron en la policlínica preoperatoria mostró que los umbrales de dolor a la presión promedio fueron menores en pacientes de sexo femenino y con dolor crónico. En voluntarios sanos, la sumación temporal mostró un aumento en la intensidad del dolor, respuesta que podría extrapolarse a la expresión normal del fenómeno de “wind-up”. En 80 % de los voluntarios sanos, la modulación condicionada del dolor resultó en un aumento del umbral de dolor a la presión con la aplicación de un estímulo doloroso heterotópico. La algometría de presión constituye un instrumento útil y práctico. La información obtenida con los test sensorial cuantitativos puede ser de gran utilidad en las Unidades de Dolor Agudo y Crónico.
Palabras clave: test sensorial cuantitativo, algometría de presión, sumación temporal, wind-up, modulación condicionada del dolor
Received: 07-01-2021
Accepted: 26-01-2022
Correspondence: Pablo Castromán Espasandín
pablocastro227@gmail.com
INTRODUCTION
In recent years, great importance has been attached to the development of objective methods for measuring the sensory system of pain transmission in humans. The quantification of pain using different types of scales (intensity, functional and psychological impact, among others) has evolved in recent years to the introduction of devices and tests allowing to explore physiological and pathophysiological aspects of pain more objectively (1). Quantitative Sensory Testing (Quantitative Sensory Testing) is a psychophysical method for quantifying the somatosensory function of the organism based on the response to mechanical, thermal or electrical controlled stimuli, including (among others) pressure algometry (PA) evaluation. This is a valid and reliable method, often used and simple to evaluate subcutaneous painful sensitivity in the local area and in distant structures, and thus allow to examine the manifestations resulting from pro- and anti-nociceptive mechanisms integrating pain modulation mechanisms (1). Temporal summation (TS) and conditioned pain modulation (CPM) integrate the dynamic tests of quantitative sensory testing (QST) (2-5).
The first of the tests allows the assessment of the ability of the painful sensory system to increase its response to repeated stimulus (wind-up response) while the second test allows the assessment of the ability to modulate local painful response to a painful stimulus applied at a distance, exploring the downward inhibitory pathway of nociception (2-4). Pressure algometry, associated with cuff pressure algometry, allows both tests to be performed with relative ease (5).
The objective of this study was to perform a preliminary experience in our University Hospital, studying quantitative sensory testing (QST) using the PA, a recently available method. The study was divided into two stages: In the first stage, the objective was to evaluate nociception in a group of preoperative patients by measuring pressure pain thresholds (PPT) by using PA. In these patients, a psychological evaluation was also performed using the hospital anxiety and depression scale (HADS) based on the relationship between these psychological disorders and pain transmission.
The objective of the second stage was to evaluate nociception by using TS and CPM in a group of healthy volunteers who are members of the Anesthesiology Service of the University Hospital.
MATERIAL AND METHODS
This is a preliminary, descriptive and interventional experience to evaluate the transmission of painful sensation by PA. In a first stage, a cross-sectional case-control study was conducted, without randomization, where the pressure pain threshold was measured in patients who attended the preoperative outpatient clinic by using PA. In a second stage, an observational study was conducted on healthy volunteers, anesthesiology residents.
The study was approved by the Ethics Committee of the Hospital de Clinicas, and it meets the criteria of Helsinski and the regulation on personal data protection. The participants signed the informed consent form after its explanation, reading and understanding. In the first stage, a sample of 58 patients was obtained consecutively, without randomization, from outpatient consultations at the Department of Anesthesiology preoperative outpatient clinic between July and November 2019. Inclusion criteria were patients over 18 years of age with confirmed non-urgent surgical treatment. The characteristics of PA were explained to these patients, and they were instructed in the HADS questionnaire, and PPT was measured. A form was populated with the personal data of each patient including: Age, sex, weight, height, type of surgery, presence of chronic pain or pain in the area to be operated on (> 3 months), pharmacological treatment of pain and mood disorders. Each patient was given the validated HADS in Spanish to be populated.
The exclusion criteria were: Age under 18 years, conditions that could affect sensory function (such as diabetic neuropathy or neurological disease), use of major opiates (at doses above 40 mg morphine equivalent/day) that could impact cognitive or sensory function, substance abuse in the last 24 months, difficulty understanding or populating the questionnaire, or refusal to participate in the study.
In a second stage, TS and CPM measurements were performed consecutively on 36 healthy resident volunteers or staff members of the Department of Anesthesiology who agreed to participate in the study. Refusal to participate in the study was considered as exclusion criteria.
Outcome variables
The PA measurement was performed with a pressure algometer (Dinator®, Argentine Industry), devise that measures the force necessary to cause painful sensations at selected points of the body previously standardized in QST studies (1). It is a measuring device that presents at one end a metallic tool of 1 cm diameter that is applied to the skin at constant speed, causing on it an increase of strength and, therefore, sensations of touch, pressure and finally pain, based on the force applied (1). The device is placed perpendicularly on the patient's skin at a constant pressure until the sensation becomes uncomfortable, then the patient warns and the application of force is stopped (Figure 1) (1). The recorded value consists of PPT expressed in Newtons (N).
In the experiments performed in the first stage, records were taken at the following points: The interdigital depression found between the thumb and index of both hands, at the level of both trapezius muscles, at half the distance between the seventh cervical vertebra and the glenohumeral joint, at the level of both quadriceps at a mid-point between the hip and knee, and finally at the level of the spine erector muscle bilaterally, 5 cm from the thorny apophysis of the third lumbar vertebra (5). Three measurements were taken per point, which were averaged, both right and left (5). The mean PPT of each individual was obtained by averaging the PPT obtained at each of the points, after averaging the measurements on the right and left sides.
Fig. 1. Application of pressure algometry in the trapezius muscle.
In the second stage, dynamic tests such as temporal summation (TS) and conditional pain modulation (CPM) were studied. In a group of these volunteers (n = 16), the TS test was performed by applying the PPT previously calculated on the right trapezius muscle over that muscle, and that value was then applied repeatedly on 10 occasions at the same site 2 minutes after PPT measurement. The pressure was gradually increased for each pulse at a rate of 2 kg/s to the determined PPT, and it was maintained for 1 seconds before being released (interstimulus interval of 1 s). The level of pressure-induced pain was assessed by volunteers on the Verbal Numerical Scale (VNS) for assessment of pain intensity from 1 to 10, in the first and tenth stimulus (5). The wind-up ratio (WUR) was calculated by dividing the value of pain intensity observed in the application of the last stimuli over the mean value of VNS obtained from the application of basal PPT (2,3).
The assessment of CPM was performed in another group of these volunteers (n = 20). A painful ischemic stimulus in the left upper limb was used as a conditioned stimulus, applying cuff pressure above 200 mm Hg of systolic blood pressure for 10 minutes, or until the subject reported pain 6/10 in the VNS. During this maneuver, volunteers were asked to perform the handgrip maneuver with a hand horn (Hand Grip Test) as shown in Figure 2 (5).
The measurement of PPT at the level of right trapezius muscle was performed immediately before and at the end of the application of the painful conditioned stimulus.
The hospital anxiety and depression scale questionnaire (HADS), validated in Spanish, was used to study anxiety and depression variables in the first stage of the study (6). It is a self-administered questionnaire, consisting of 14 questions, 2 subscales of 7 items each. The intensity or frequency of the symptom at each item is evaluated on a 4-point Likert scale (range 0-3). The anxiety subscale corresponds to odd items, whereas the depression subscale corresponds to even items, with a score range in each subscale of 0 to 21 and 0-42 for the overall score. The higher the score, the more likely the patient is to have anxiety and depression. Anxiety: The maximum score range is 21 points. The results are: “unlikely” for those under 8 points, “possible cases” those over 8, but under 11, and “probable cases” with scores over 11. The same diagram is used for the diagnosis of depression. The scale has high internal consistency (Cronbach's alpha between 0.83 and 0.85), high reliability test retest (r = 0.75) and sensitivity ranges between 0.74 and 0.84, specificity from 0.78 to 0.80 (6).

Fig. 2. A measure of conditioned pain modulation. The image shows the ischemic painful stimulus by insufflation of the pressure cuff above blood pressure and the concurrent application of the Hand Grip maneuver. After the maneuver, PPT is measured at the level of the trapezius muscle and compared with the baseline measurement.
Statistical analysis
The data were analyzed using the GraphPad Prism software version 7, and presented as the mean, and its standard deviation for the quantitative variables and as the absolute value and percentage for the qualitative variables. The normal distribution of the data was corroborated by the use of the Shapiro-Wik test for all the studied variables. For the first stage of the study, differences in PPT were compared between the pain group and the pain-free group, as well as between the sexes, using the Student’s t test for independent samples. The differences between the proportion of patients with pain between the sexes were compared with the Fisher test. The correlation between mean PPT and body mass index (BMI) was calculated using a Pearson correlation test. The number of patients with presumptive diagnosis of anxiety and depression in the total number of patients evaluated was expressed as a percentage. Values equal to or greater than 8 were considered as the cut-off point for the diagnosis of both disorders. The frequency of occurrence of anxiety and depression was contrasted using the Fischer test for comparison of proportions. The Chi square test was used to evaluate differences in frequency of anxiety and depression based on sex. The relationship between the anxiety and depression scores obtained by HADS and PPT was evaluated by using the Pearson's correlation coefficient.
In the second stage, the Student’s t test for dependent samples was used to analyze changes in the TS and CPM variables in the study group of healthy volunteers. A p value less than or equal to 0.05 is considered statistically significant.
RESULTS
First stage
The 58 patients studied in the first stage were 25 women and 33 men, with a mean age of 58 ± 11 years, and a BMI of 27.9 ± 6. The reason for excluding patients observed at this stage was the refusal to participate in the study and in one case, the inability to read the anxiety and depression questionnaire.
The distribution of the types of surgery proposed was as follows: General surgery 42 % (n = 24), ophthalmology 17 % (n = 10), urology 17 % (n = 10), gynecology 8.6 % (n = 5), ENT surgery 8.6 % (n = 5), spine surgery 3.4 % (n = 2), kidney transplant 1.7% (n = 1) and plastic surgery 1.7% (n = 1).
A total of 18 (31%) out of the 58 patients reported chronic pain prior to surgery in different topographies or at the surgical site (pain group). Table I shows the causes of pain found in this group.
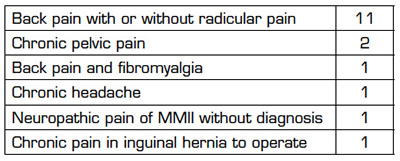
Table II shows the means of the PPT in hand, trapezius, quadriceps and lumbar, right and left, both in the pain group and in the pain-free group.
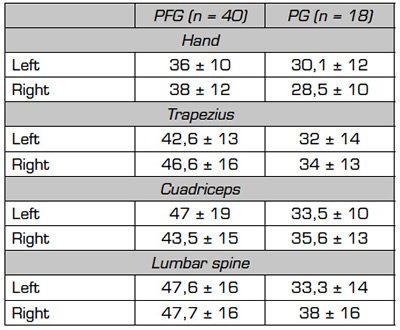
*The unit of measurement of MPPT is newtons.
A lower PPT was observed in the group of patients with a history of chronic pain at all the studied points, statistically significant (t-test for independent samples, p < 0.05). No statistically significant differences were found in the PPT taken between the right or left side at any of the points.
Figure 3 shows the PPT in the different regions studied, averaging the measurements made on the right and left side comparing the preoperative patients without pain and with pain. Patients with some type of preoperative chronic pain showed lower PPT at all points assessed than those with no history of chronic pain, these differences were statistically significant in all cases.
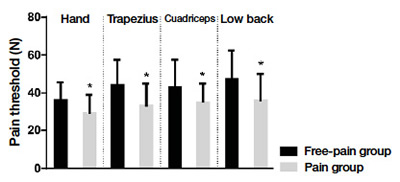
Fig. 3. Mean PPT of the four regions analyzed. Comparison of pain-free and pain patients.
*p < 0.05 t-test for independent samples.
The mean PPT of the pain group was 32.7 ± 10 N, while that of the pain-free group was 42 ± 11.7 N, this difference being statistically significant (p < 0.05, t-test for independent samples).
Mean PPT in female patients was 36.6 ± 9 N, whereas in male patients it was 48 ± 11 N. This difference is statistically significant (p = 0.001, t-test for independent samples). It is important to note that there were no statistically significant differences in the proportion of patients with pain between women and men when using the Fisher Test.
No linear correlation was found between mean PPT and BMI using a Pearson test (R = 0.07). Out of the total of patients evaluated at the preoperative consultation, 15 patients (25.8%) had values greater than or equal to 8 for anxiety and 7 patients (12%) had values greater than 8 for depression. Comparing patients with anxiety or depression among patients with a history of chronic pain, 7 out of 18 (38.8%) had anxiety and 2 out of 18 (11.1%) had depression; whereas anxiety was found in 8 out of 40 (20%) and depression was found in 5 out of 40 (12.5%) in those without a history of chronic pain. Although anxiety was more frequent in the pain group, this difference was not statistically significant using a Fischer Test (p = 0.19). The presence of anxiety was associated with a lower mean PPT. The mean PPT of patients who had scores greater than 8 in HADS was 36 ± 12 N, while those who had no elements of anxiety was 44 ± 12 N, this difference being statistically significant (p = 0.05). In the group of patients who did not have a history of chronic pain (69% of those studied), those who had higher levels of anxiety and/or depression according to the HADS had lower mean PPT than those without pain and without high levels of anxiety or depression (37.3 ± 4 versus 45.2 ± 2.4), but this difference did not reach statistical significance.
Second stage
In the volunteers in whom the TS test was performed, it was found that the level of pain in the EVN went from 4.1 ± 1 with the initial stimulus to 6.5 ± 1.5 with the final stimulus, implying 2.4 points of increase (58%). This difference was statistically significant by applying a T test for dependent samples (p = 0.0001) (Figure 4). The calculated Wind-Up Ratio (WUR) (percentage correlation of the TS) resulted in a value of 1.58.
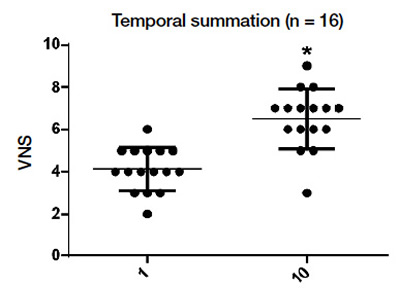
Fig. 4. VNS in the first and tenth stimulus. p < 0.0001, t-test for dependent samples.
In the remaining 20 volunteers in which the CPM test was performed, the initial mean PPT at the right trapezius level was 63 ± 27 N. After the conditioned pain stimulus was performed, That was reached in a mean of 45 ± 36 seconds after the start of the test, the PPT recorded in the right trapezius was 72 ± 28 N. There was an increase in PPT on average of 9 N (14.2%). This difference was statistically significant by applying a T Test for dependent samples (p = 0.02) (Figure 5). Of the total number of volunteers, 16 presented modulation and 4 did not have the expected response (20% failure).
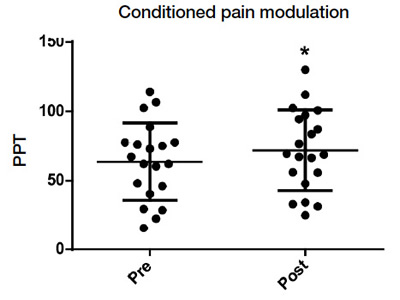
Fig. 5. Pre and post PPT in CPM. *p = 0.02, t-test for dependent samples.
DISCUSSION
QST are a set of tests used to quantify the somato-sensory function of the organism based on the response to controlled stimuli. QST allow a greater understanding of the mechanisms involved in pain, identify individual differences in pain perception, evaluate its mechanisms, either at the central or peripheral level, identify subgroups of patients, establish populations at risk of developing chronic pain, assess the efficacy of pharmacological or non-pharmacological treatments and predict the most recommended therapy based on the tests (1). In our midst we had no previous experience with these tests. The objective of this preliminary experience was to familiarize ourselves with this assessment and adapt it to our clinical reality.
The PPT values observed in the present study are significantly lower in the group of patients with a history of chronic pain, and are consistent with those found by other authors (7). Blumenstiel found a higher pressure sensitivity in patients with chronic lower back pain compared to healthy volunteers; a similar result observed Jason (8,9). The mean PPT found in this research was significantly lower in female patients than in male patients. Rolke reports similar results in healthy volunteers, and argues that this difference may be linked to different pain processing or the incidence of psychological factors (10). Skovbjerg, in a study conducted on a sample of the general adult population, also found a statistically significant association between decreased PPT values and female sex (11). Higher sensitivity to painful pressure stimulation has been consistently observed in women compared with men in several studies (12). This author also found an interaction between the decreased PPT index and the increase in body mass, which was not observed in the present study.
Regarding the psychological factors assessed for anxiety or depression, the percentage of anxiety (25.8 %) present in the sample of patients evaluated in the preoperative period, which is significantly higher than the percentage of depression, but with no statistically significant difference, is highlighted. The presence of anxiety evaluated by using the HADS in patients who consult for preoperative assessment is a relatively frequent element, which we have found in our Anesthesiology Service (13).
For PPT values and their relationship to anxiety and/or depression, in patients who did not have anxiety or depression measured by HADS, higher mean UDP was observed than in patients with anxiety. It would seem that anxiety itself is capable of affecting the measurement of the pressure thresholds measured by algometry, decreasing them. Othman, in a systematic review of somatosensory function alterations in patients with joint pain, found a significant association of anxiety, depression, and catastrophism with several of the QST measures, including PPT (14). Rudhi found that anxiety lowers pain thresholds and suggests that it may have a role in determining central hypersensitivity (15). In any case, these data support the need to assess the psychological aspects identified when conducting studies on QST.
Because of our lack of experience with QST, and because dynamic tests such as TS and CMD can cause discomfort to patients, it was preferred to perform them in this preliminary experience in a second stage, with healthy volunteers. rather than for patients who attended the preoperative assessment visit.
In the case of TS, the increase in pain from the first to the last stimulus is about 1.6 times in most studies, but in the presence of central sensitization, TS may be exaggerated in amplitude and extent (2.4,5). In the present preliminary work, TS was successfully induced and showed a significant increase between the first and last stimulus. The calculated WUR resulted in a value of 1.58. Similar results are reported by Markuzzi in a pain-free population, in which a WUR of 2.2 on the back was recorded (16). This author, when studying a population with acute pain, found an increase in TS in relation to control with healthy volunteers (16).
In relation to CPM, the reduction of the stimulus test implies that the downward inhibitory pathway is intact or functional, a situation that was found in 80 % of the volunteers investigated in this study in which a 14.2 % increase in PPT was recorded (16). Pud states that the magnitude of this increase mentioned in several studies is 25 % of the pain thresholds (17).
Just as certain psychological factors are reported as predictors for lower back pain, a deficit in conditioned pain modulation can predict the propensity to develop chronic pain (18). Edwards argues that normal individuals with inefficient CPM would be more likely to develop chronic painful syndromes (19). In that situation could be healthy individuals, in which the expected response is not found, an absolutely speculative assertion.
The present study, however, has many limitations in interpreting the results. The objective of this preliminary experience was to familiarize themselves with the QST and adapt them to our clinical reality, so the tests used were applied with the concept of reducing the discomfort of the volunteers studied, facilitating their participation, and adapting them to their possible routine application in clinical practice. For this purpose, the tests were applied with some differences in relation to the original descriptions and therefore these modifications may have influenced the final results obtained. The validity of these tests depends on the training of the personnel who perform them and the follow-up of a strict protocol in their application. Although these tools have been used in experimental studies, there is still a lack of studies to standardize protocols to be applicable to the clinic and, for example, to establish normal value tables in a healthy population. The PPT values recorded in this preliminary experience could serve as a reference for future tests, since, although studies with reference values are available, these correspond to measurements performed under different conditions and exploring another type of localization of stimuli (5,7,8).
Another purpose of the experience presented was to make contact with more objective methods for the assessment of nociception in humans. However, with the tocarriols used it is possible to objectively quantify the nociceptive stimulus, not the response of the individual who is still evaluated through subjective scales of assessment of the intensity of pain.
Interestingly, a recent review (2021) on outcome assessment methods in clinical trials on pain did not mention QST in the extensive presentation of tools proposed by the authors (20).
Another methodological limitation of the present experience was the measurement of TS and CPM only in healthy volunteers, we consider that it would be interesting to assess patients with and without pain in future. We must also point out the possibility of bias at this stage, where the population of healthy volunteers has the same characteristics with regard to age and has knowledge of the subject matter to be studied, which could influence the results, which compromises the external validity of such study.
CONCLUSION
The application of PA in patients who attended the preoperative outpatient clinic showed that the mean PPT was lower in those who had a history of some type of chronic pain in their personal pathological history. Mean PPT was lower in women than in men. In healthy volunteers in which TS was assessed by using PA, a statistically significant increase in pain intensity from the first stimulus to the end was obtained as a normal expression of the sensitization phenomenon. In 80 % of healthy volunteers in whom the CPM test was applied, this was positive, i.e. an increase in PPT was found with the application of a painful heterotopic stimulus, as an expression of the function of the downstream analgesia systems. Future studies will allow the study of the incidence of factors such as sex, age or body mass on dynamic studies.
Information obtained with QST can be very useful in pain units, allowing, among others, to identify differences in pain perception, establish risk groups for developing chronic pain, and predict response to possible treatments. It seems important to evaluate the psychological aspects of the individuals studied on some type of validated scale, when studying QST.
ACKNOWLEDGMENTS
To Professor Dr. Héctor Piriz, for his persevering insistence to develop a model of clinical-basic research, which allows the pathophysiological study of nociception and pain in humans in our country.
REFERENCES