DOI: 10.20986/resed.2021.3825/2020
ORIGINAL
POSTOPERATIVE KETAMINE EFFICACY IN PATIENTS RECEIVING CHRONIC OPIOIDS UNDERGOING SPINAL SURGERY
EFECTIVIDAD DEL USO DE KETAMINA PERIOPERATORIA EN PACIENTES SOMETIDOS A CIRUGÍA DE RAQUIS EN TRATAMIENTO CRÓNICO CON OPIOIDES
U. Rodríguez Rivas1
E. Vilà Barriuso1
L. Trillo Urrutia1
M. Soldevilla García1
J. García Álvarez1
1Servicio de Anestesiología y Reanimación. Parc de Salut Mar. Barcelona, España
ABSTRACT
Introduction: The number of patients receiving chronic opioids undergoing spinal surgery has increased lately. Elevate records in visual analog scale (VAS) and opioid consumption are higher in this group of patients.
Material and methods: Following the recommendations of the American Pain Society (APS), a new intra and postoperative analgesic protocol based on the use of ketamine was designed in 2018. Intraoperatively, a bolus of 0.5 mg/kg of ketamine was administered, followed by a dose infusion of 0.2 mg/kg/h until the surgical wound was closed. During the first 48 postoperative hours, a patient-controlled analgesia pump (PCA) of morphine-ketamine was maintained along with a multimodal analgesia regimen with paracetamol and dexketoprofen. An effectiveness analysis comparing the new protocol (ketamine group) with the previous one (control group), based on the use of tramadol 100 mg / 6h or PCA morphine, was done. During the first 48 postoperative hours, NVS records, need of rescue analgesia, morphine bolus or continuous morphine infusion (control group) or ketamine morphine infusion (ketamine group) were analyzed.
Results: The patients in the ketamine group had lower NVS records than those in the control group during the first two postoperative hours (p = 0.001) and lower morphine rescues needs on the second postoperative day (p = 0.003). The need for continuous morphine-ketamine perfusion was significantly lower than the need for continuous morphine perfusion on the control group (p = 0.011).
Conclusion: The protocol based on the use of ketamine, managed to improve the control of postoperative pain and significantly reduce the consumption of opioids in the first 48 hours after the intervention.
Key words: Pain, postoperative, ketamine, surgery, spine.
RESUMEN
Introducción: El número de pacientes en tratamiento con opioides de forma crónica sometidos a una cirugía espinal ha aumentado en los últimos años. Los registros de dolor mediante la escala visual analógica (EVA) y el consumo de opioides durante el postoperatorio son más elevados en esta clase de pacientes.
Material y métodos: Siguiendo las recomendaciones de la American Pain Society (APS), en 2018 se diseñó un nuevo protocolo analgésico intra y postoperatorio basado en el uso de ketamina. En el intraoperatorio, se administró un bolus de 0,5 mg/kg de ketamina, seguido por una perfusión a dosis de 0,2 mg/kg/h hasta el cierre de la herida. Durante las 48 horas postoperatorias, se mantuvo una bomba de analgesia controlada por el paciente (PCA) de morfina-ketamina junto con un régimen de analgesia multimodal con paracetamol y dexketoprofeno. Se realizó un análisis de la efectividad del nuevo protocolo (grupo ketamina) comparándolo con el protocolo seguido el año anterior (grupo control), basado en el uso de tramadol 100 mg/6 h o PCA de morfina. Se analizaron los registros de dolor mediante la escala verbal numérica (EVN) durante las primeras 48 horas postoperatorias, la necesidad de administración de bolus puntuales de morfina y la necesidad de iniciar una perfusión continua de morfina (grupo control) o morfina ketamina (grupo ketamina).
Resultados: Los pacientes del grupo ketamina presentaron EVN inferiores a los del grupo control durante las dos primeras horas postoperatorias (p = 0,001) y menores necesidades de rescates de morfina en el segundo día postoperatorio (p = 0,003). La necesidad de perfusión continua de morfina-ketamina fue significativamente inferior a la necesidad de inicio de perfusión continua de morfina en el grupo control (p = 0,011).
Conclusión: El protocolo basado en el uso de ketamina consiguió mejorar el control del dolor postoperatorio y reducir de forma significativa el consumo de opioides en las primeras 48 horas tras la intervención.
Palabras clave: Dolor, postoperatorio, ketamina, cirugía, espinal.
Correspondence: Uxía Rodríguez Rivas
60533@parcdesalutmar.cat
Received: June 16, 2020
Accepted: March 22, 2021
INTRODUCTION
Patients undergoing spine surgery experience moderate-severe pain during the postoperative period (1). VAS pain intensity records typically range from 5 to 8, depending on the procedure performed (1,2). At our center, 20 % of the patients who underwent surgery are receiving chronic opioid treatment before surgery. This incidence is similar to that described in the literature (3,4).
In the first 48 postoperative hours, patients on chronic opioid therapy have higher morphine requirements and VAS records (5). The use of non-opioid adjuvant drugs (6) is recommended to optimize its analgesic treatment. Low-dose ketamine is useful in this context (6,7).
In 2018, following the guidelines of APS (6), our center decided to change the postoperative analgesic protocol for patients on chronic opioid treatment scheduled for spine surgery. During the intraoperative period, the use of continuous ketamine infusion (CI) at low doses was protocolized. In the first 48 postoperative hours, the use of a PCA with morphine-ketamine was chosen to replace the protocol used up to that time, in which tramadol (100 mg/6 h) or a PCA with intravenous morphine was prescribed. In both protocols, multimodal analgesia with paracetamol and dexketoprofen prescribed is also considered.
The main objectives of this analysis were to compare pain intensity assessed using VNS and rescue opioid consumption in the first 48 postoperative hours between two cohorts of patients. One cohort consisting of patients who received either tramadol or morphine PCA (control group) and another cohort consisting of patients who received intraoperative ketamine with a PCA regimen with morphine-ketamine (ketamine group) in the first 48 postoperative hours.
MATERIAL AND METHODS
This study is a retrospective efficacy analysis of the new analgesic protocol implemented in the Anesthesiology Service of the Hospital del Mar in Barcelona compared with the previous protocol. No confidential data from the patient’s medical records is published.
Inclusion and exclusion criteria
All patients treated with strong opioids or oral tramadol doses equal to or above 200 mg/24 h, for 6 weeks or more before any type of back surgery in 2017 and 2018 were included in the analysis.
Patients who did not successfully complete the analgesic protocol were excluded.
Rescue analgesia in the postoperative intensive care unit (POICU): Bolus of 2 mg morphine i.v. until a VNS < 3 is obtained as a first option, or continuous infusion of morphine at 1 ml/h is initiated as a second option.
Rescue analgesia in the hospitalization unit: Bolus of subcutaneous morphine (s.c.)/4 h at doses of 0.01 to 0.05 mg/kg until a VNS < 3 is achieved.
Rescue analgesia at the POICU: Bolus of 2 mg morphine i.v. until a VNS < 3 is reached as the first option, or the initiation of continuous morphine-ketamine infusion at 1 ml/h as the second option.
Rescue analgesia in the hospitalization unit: Morphine bolus s.c./4 h at doses of 0.01 to 0.05 mg/ kg until a VNS < 3 is achieved.
Assessed variables
All data were collected from the medical and nursing records of the patients’ computerized medical records. The following demographic data were analyzed: Sex, age, and preoperative diagnosis. Regarding the preoperative analgesic treatment, the following data were collected: The type of opioid and the dose administered, the use of concomitant medication, and the performance of invasive analgesic techniques. The following data were collected on the surgical procedure: Performed surgical technique (laminectomy, arthrodesis, rearthrodesis, material removal, etc.), surgical time, level and spaces operated, and intraoperative opioid used. During the postoperative period, VNS records were collected at 2 h after the end of the surgery, and during 48 h postoperative period (evaluated every 8 h), the type of opioid prescribed, its dose, and the administration of rescue analgesia. Psychomimetic symptoms, impaired consciousness, respiratory depression, and nausea or vomiting were also reported.
Statistical analysis
The SPSS statistical package version 17 for Windows was used for statistical analysis. Mean and standard deviation were used in the description of continuous variables. The number and percentage of patients by response category were used for the description of categorical variables. Statistical techniques were used to ensure compliance with statistical assumptions before comparative testing. If the established assumptions were not met, the corresponding non-parametric tests were used. Comparative analyzes were performed only for categorical variables. The Chi-square test was applied in comparisons with the nominal dependent variable and the Mann-Whitney U test compared with the ordinal dependent variable. A statistical significance level of 0.05 was set for all statistical tests.
RESULTS
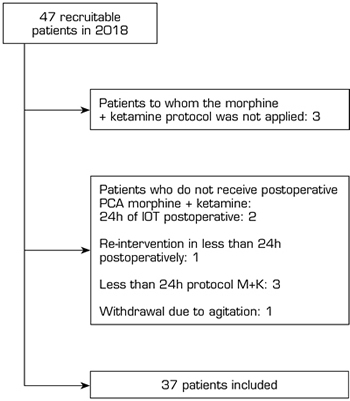
A total of 43 patients were included in the control group. In the ketamine group, 37 out of the 47 patients undergoing chronic opioid treatment in 2018 were included. Ten patients were excluded: Morphine-ketamine (M-K) protocol was not applied in 3 patients, and it was not fully applied in 7 patients (Figure 1).
Fig. 1. Flow chart of recruitable and included patients
Demographic characteristics are similar in both groups (Table I). The most frequent preoperative diagnoses were canal stenosis and disc hernia. The most frequent surgical technique was arthrodesis. A total of 50 % of patients underwent spinal surgery for the first time.
Table I. Demographic data
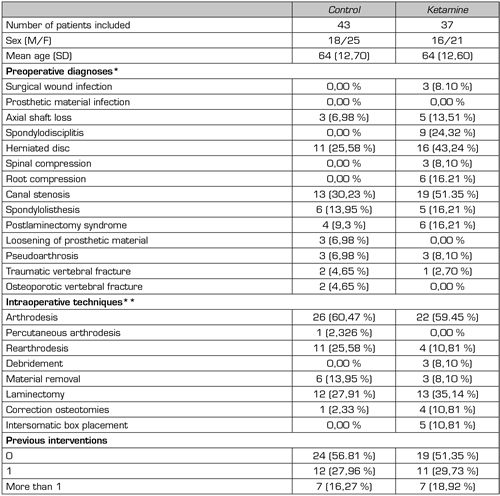
*Diagnostics are not exclusionary. **Surgical techniques are not exclusionary
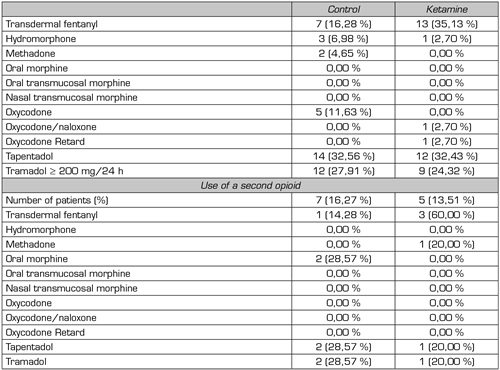
Tramadol, tapentadol, and transdermal fentanyl were the most preoperatively prescribed opioids in both groups. The percentage of patients receiving concomitant treatment with two opioid drugs was similar in both groups: 16.27 % control, 13.51 % ketamine (Table II).
Table II. Preooerative opioid treatmen
The mean preoperative morphine dose is expressed in oral milliequivalents (mEq) of morphine and was calculated according to the sources in Annex I. In the control group, patients received a mean dose of 75.93 mEq, with a standard deviation (SD) of 59.97 mEq. In the ketamine group, the mean was 50 mEq (SD 71.60 mEq).
Annex I. Table of opioid equivalence
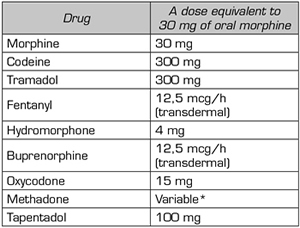
Source: O’Brien T, Christrup LL, Drewes AM, Fallon MT, Kress HG. European Pain Federation position paper on appropriate opioid use in chronic pain management. Eur J Pain. 2017;21(1):3-19. DOI: 10.1002/ejp.970.
*Use of 5:1 for conversion from methadone to oral morphine. (Source: Mercadante S, Casucio A, Calderone L. Rapid switching from morphine to methadone in cancer patients with poor response to morphine. J Clin Oncol. 1999;17[10]:3307-12. DOI: 10.1200/JCO.1999.17.10.3307.).
Preoperative, all patients analyzed performed multimodal analgesia combining at least one opioid with another analgesic drug (Table III). In both groups, more than one-third received neuropathic pain medication.
Table III. Other analgesic drugs and preoperative invasive analgesic techniques
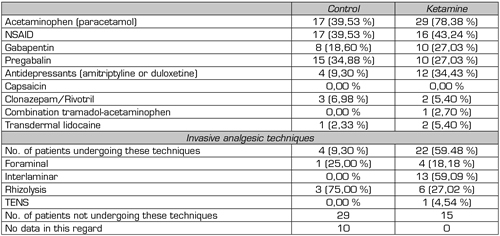
The difference in the use of invasive analgesic techniques (control 8.5 % vs. ketamine 100 %) is not analyzable. For most patients in the control group (67 %), no data is available due to the absence of records in the electronic medical record.
During the intraoperative period, fentanyl was the most commonly used opioid (ketamine group 82.6 %, control group 93 %). The doses used ranged from 400 to 1100 mcg in both groups. The dosage varies depending on the intervention performed (e.g., discectomy vs. multilevel arthrodesis with osteotomies) and the required intraoperative opioid requirements according to the criteria of each anesthesiologist responsible for the surgery.
Figure 2 shows VNS records during the first two hours of the postoperative period, from 2 to 24 hours, and during the second day of the postoperative period. Except for the first 2 postoperative hours, during which the VNS of the ketamine group are decreased (p = 0.001), no differences between the two groups were found. Figure 3 shows the need for rescue morphine bolus over the same periods. There are statistically significant differences during the second postoperative day (p = 0.003) in favor of the ketamine group.
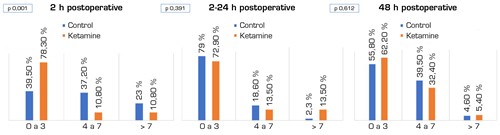
Fig. 2. Levels of NVS during the 48 postoperative hours. Mann-Whitney U test
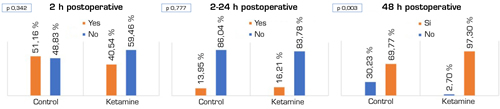
Fig. 3. Percentage of patients who needed or did not need a morphine bolus. Chi-square test
From the patient’s electronic medical record, dose data could only be obtained for morphine bolus administered during the first 24 hours postoperatively. In the control group, a mean of 2.47 mg morphine i.v. (2-10 mg) was administered during the first 2 hours postoperatively. Between the first 2 and 24 hours, an average of 0.49 mg (0-10 mg) was administered. In the ketamine group, an average of 1.69 mg morphine i.v. (0-8 mg) was administered during the first 2 hours. Between 2 and 24 hours, a mean of 0.62 mg (0-8 mg) was administered.
Regarding the need for continuous infusion, either morphine in the control group or morphine-ketamine in the ketamine group, patients in the ketamine group had significantly lower needs (Figure 4).
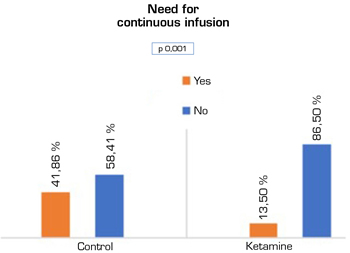
Fig. 4. Need for morphine infusion from admission to resuscitation to 48 postoperative hours. Chi-square test
Concerning complications from analgesic treatment, none of the patients in the control group had psychomimetic symptoms, only 1 patient had postoperative nausea or vomiting (PONV), 6 patients had decreased level of consciousness (sleepiness), and 1 patient had bradypnea. In the ketamine group, 1 patient presented dysphoria and 3 patients presented PONV. None of the patients in the ketamine group had respiratory or level of consciousness changes.
DISCUSSION
With the implementation of the low-dose ketamine-based analgesia protocol in 2018, we have decreased the need for rescue opioids in our center and improved pain management in the first two postoperative hours. No higher incidence of adverse events has been recorded.
The number of patients with back pain on opioid therapy has increased in recent decades (8,9,10). Multimodal analgesia is the most correct approach, both pre-and postoperative (6,11). At subanesthetic doses, ketamine has been shown to decrease the requirements of postoperative opioids, especially in these types of patients (6,7,12,13).
The results found in our analysis are comparable to the results published by Loftus et al. (14) and Nielsen et al. 15. Both clinical trials demonstrated a decrease in postoperative opioid use and improved pain control in patients on chronic opioid therapy.
Similar to Nielsen et al., we decided to include patients treated with tramadol in the analysis. Although the minimum opioid dose at which a patient may have tolerance or secondary hyperalgesia is unknown, doses below 40 mg of oral morphine have been found to cause them (16).
A subanalysis was performed in the study conducted by Nielsen et al. to clarify whether patients with higher doses of morphine in the preoperative period had a higher decrease in morphic consumption in the postoperative period. It is noted that the reduction is higher with doses above 36 mEq oral morphine. In our study, no such analysis was performed because of the small number of patients included.
The use of high-dose opioids during the intraoperative period results in hyperalgesia and tolerance during the first two postoperative hours (17,18,19). However, continuous intraoperative ketamine infusion may prevent the hyperalgesia component by acting on NMDA receptors (20). In our center, intraoperative opioid needs may reach 1100 mcg of intravenous fentanyl. It has not been analyzed whether the main factor determining the need for such high doses is the largest surgical aggression or whether chronic opioid treatment is a relevant factor. In patients in the ketamine group, despite having intraoperative opioid needs similar to those in the control group, VNS records are significantly lower during the first two postoperative hours than in the control group. The effect of infusion at subanesthetic doses of ketamine during surgery may justify this finding.
In our center, patients are not moved in the first 24 postoperative hours. Pain management in this period is acceptable in both groups. However, sitting and early motion begins at 48 hours. In the case of the ketamine group, patients have better baseline analgesic control, requiring fewer rescue opioids. Maintaining ketamine in this period may be key because nociceptive stimulation is again of high intensity (12).
This analysis has some limitations. During the postoperative period, it was not possible to record the number of morphine PCA bolus or morphine + ketamine PCA bolus administered to each patient. Nor are the doses of rescue morphine administered in the hospital ward. We also do not know whether the VNS records are regarding moving or resting.
CONCLUSIONS
The use of ketamine during intraoperative and the first 48 postoperative hours in patients with chronic opioid treatment undergoing spinal surgery decreases the need for postoperative opioids and improves pain management in the first 2 postoperative hours. In the future, a prospective observational study would allow us to understand pain control fully, the need for rescue opioids, the degree of satisfaction, and the rate of complications in patients treated with ketamine. It would be interesting to know the effect of this drug after 6 and 12 months of the intervention because the use of intraoperative ketamine could decrease long-term pain and its chronification.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
REFERENCES