doi.org/10.20986/resed.2025.4171/2024
ORIGINAL
Rative study between psoas compartment block versus local anesthesia with remifentanil sedation for endovascular repair of abdominal aortic aneurysm (evar): a prospective randomized study
Estudio comparativo entre bloqueo del compartimiento del psoas versus anestesia local con sedación con remifentanilo para la reparación endovascular del aneurisma aórtico abdominal (evar): un estudio prospectivo aleatorizado
Wesameldin A. Soltan1
Osama M. Asaad1
Ayman A. El Sayed1
1Department of Anesthesia, ICU & Pain management, Faculty of Medicine, Menoufia University, Menoufia, Egypt
ABSTRACT
Background: This study aims to evaluate the safety and effectiveness of psoas compartment block compared to local anesthesia with remifentanil sedation for endovascular abdominal aortic aneurysm repair.
Methods: This prospective, randomized, single-blinded study included 30 patients divided into two equal groups. Fifteen patients underwent elective endovascular repair under psoas compartment block (PCB group), and fifteen underwent the procedure under local anesthesia with remifentanil infusion (LR group).
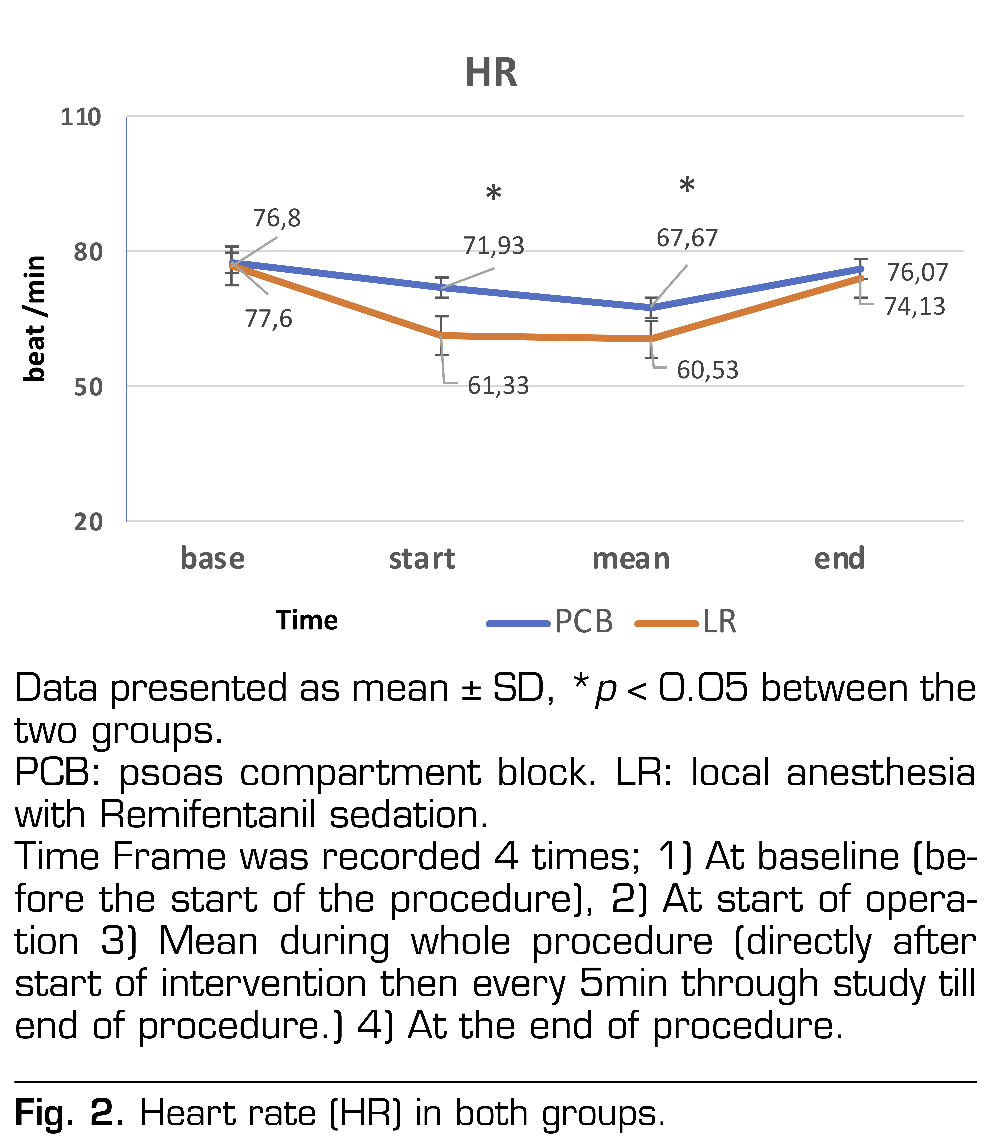
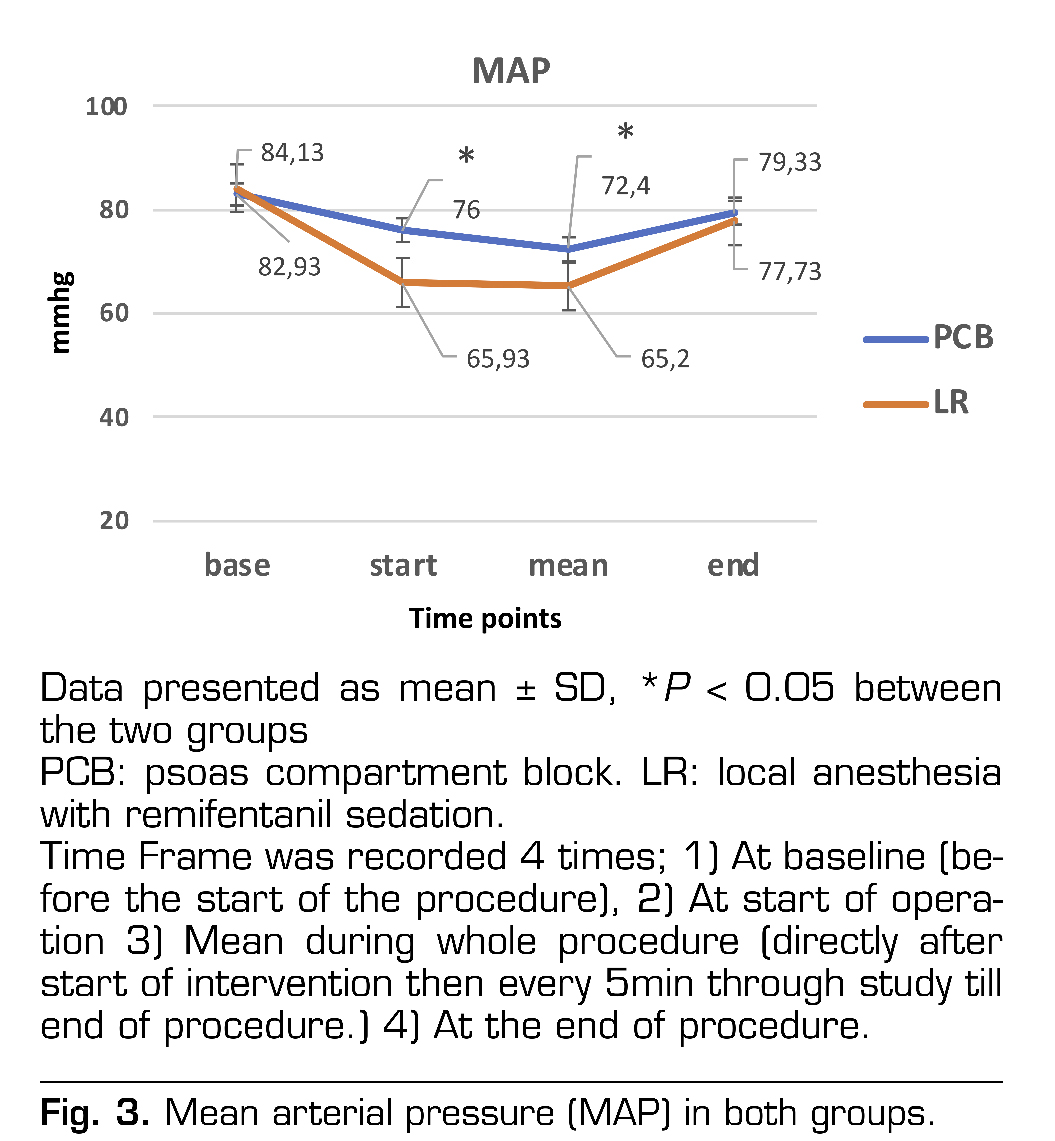
Results: The mean VAS scores were significantly lower in the LR group compared to the PCB group (P < 0.001). Ramsay Sedation score showed statistically significant deep sedation in LR group on comparison to PCB group (P< 0.001). In patients under remifentanil sedation (LR group), the heart rate and mean arterial blood pressure decreased significantly after induction of anesthesia and stayed low but without any clinical significance throughout the procedure (P< 0.001).
Conclusions: This study demonstrates that endovascular abdominal aortic aneurysm repair under either psoas compartment block or local anesthesia with remifentanil sedation is a safe and effective procedure, with favorable perioperative outcomes.
Key words: Psoas compartement block, remifentanil, endovascular aortic aneurysm repair
RESUMEN
Antecedentes: Evaluar la aplicabilidad del bloqueo del compartimiento del psoas para la reparación endovascular del aneurisma aórtico abdominal en comparación con la anestesia local con sedación con remifentanilo.
Métodos: Estudio prospectivo, aleatorizado, simple ciego sobre 30 pacientes divididos en 2 grupos iguales, 15 pacientes fueron sometidos a reparación endovascular electiva de aneurisma de aorta abdominal bajo bloqueo del compartimento del psoas (grupo PCB), mientras que otros 15 pacientes fueron operados bajo anestesia local con infusión de remifentanilo (grupo LR).
Resultados: Los valores medios de VAS mostraron mejores valores estadísticamente significativos en el grupo LR en comparación con el grupo PCB (p < 0,001). La puntuación de sedación de Ramsay mostró una sedación profunda estadísticamente significativa en el grupo LR en comparación con el grupo PCB (p < 0,001). En pacientes bajo sedación con remifentanilo (grupo LR), la frecuencia cardiaca y la presión arterial media disminuyeron significativamente después de la inducción de la anestesia y se mantuvieron bajas pero sin ninguna importancia clínica durante todo el procedimiento (p <0,001).
Conclusiones: El presente estudio demostró que la reparación endovascular del aneurisma de la aorta abdominal bajo bloqueo del compartimento del psoas o anestesia local con sedación con remifentanilo es un procedimiento seguro y eficaz para el tratamiento de los aneurismas de la aorta abdominal, con mejores resultados perioperatorios.
Palabras clave: Bloqueo compartimental del psoas, remifentanilo, reparación endovascular de aneurisma aórtico
Correspondencia
Wesameldin A. Soltan
wesamsultan@med.menofia.edu.eg
Recibido: 17-09-2024
Aceptado: 06-12-2025
INTRODUCTION
Abdominal aortic aneurysms (AAA) account for about 65 % of all aneurysms of the aorta and 95 % of them lie below the renal arteries (1). Recently, the management of aortic aneurysm has changed from the traditional open technique to minimally invasive incisions and even percutaneous techniques (2).
Endovascular aortic aneurysm repair (EVAR) was first introduced in 1991 (3), and lately is progressively being used for AAA repair (4). When compared with open surgical approach, EVAR is considered superior, being less invasive, less blood loss, less cardiovascular drawbacks, minimal metabolic stress response, shorter hospital stay and earlier ambulation (5). However, EVAR is considered costly and its long-term success is still not clear (6).
EVAR through surgical cutdown to the common femoral arteries (CFA) can be done under local anesthesia with sedation, general or regional anesthesia (7,8). Several single and multicenter researches have evaluated the results with these anesthesia techniques for EVAR, with varying outcomes (9,10,11). Based on the European Society for Vascular Surgery guidelines, the use of local anesthesia with sedation for EVAR is applicable and well tolerated, while regional or general anesthesia could be used only if local anesthesia is contraindicated (12).
Although, painful skin incision was reduced by local anesthesia given at the site of entry, sedative/analgesic cover is mandatory to achieve a comforTable level for the patient, allowing surgeon/patient communication, without interfering with hemodynamics or the cardiocirculatory system. The key point of this kind of operation is that pain occur in certain moments separated by pain free intervals, so skilled anesthesiologist can guess the pain occurrence points and prepare himself to prevent it with analgesics (13).
It is obvious that there is the need for a minimally invasive anesthesia with a minimally invasive surgical technique. New drugs, like remifentanil, with an ultra-short half-life and being potent opioid, succeed to accomplish this minimal invasive anesthesia, as shown by other studies (14).
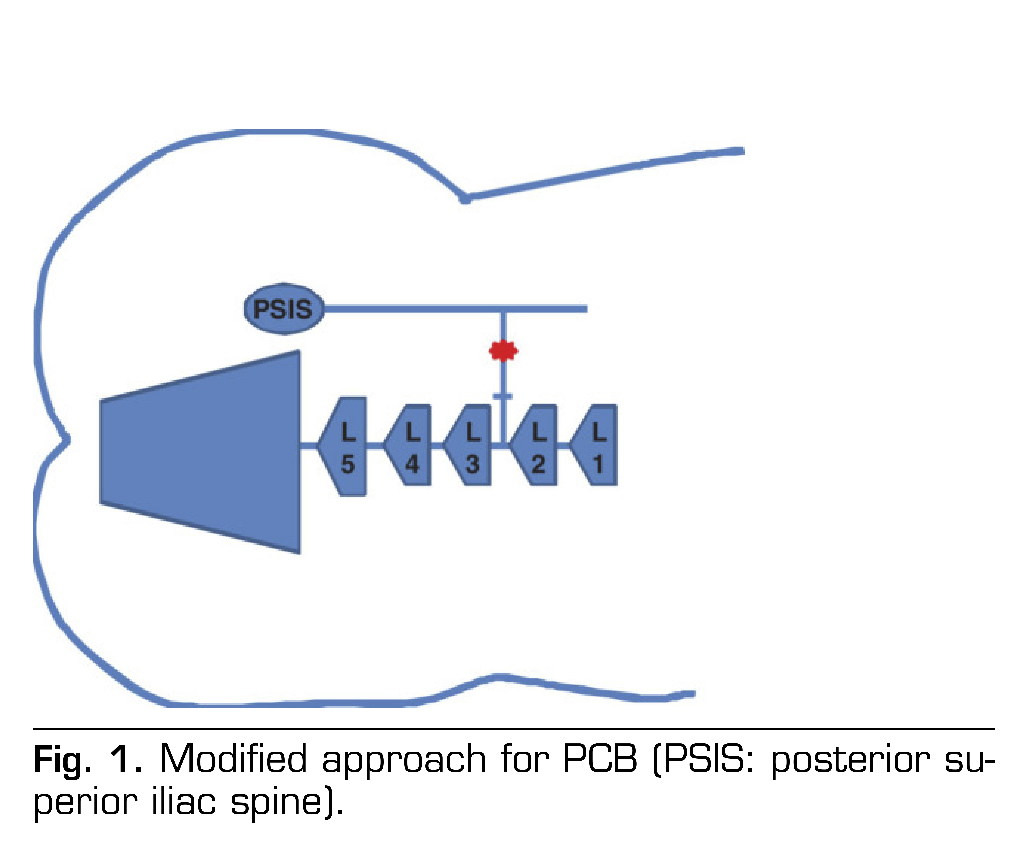
Anatomical, imaging and clinical researches suggest psoas compartment block (PCB) (lumbar plexus block) made at L2–L3 level has a high probability to include L1–L2 roots, and therefore considered a good choice for inguinal surgery (15,16). We applied the modified access technique described before by Mokini and his colleges (17) for PCB as a real alternative for infiltration of local anesthetic in patients undergoing EVAR.
Aim of the work was to demonstrate safety and effectiveness of psoas compartment block compared to local anesthesia with remifentanil sedation for EVAR. The primary endpoint of this study was the extent of success for both anesthetic approaches to control pain intraoperatively measured by Visual Analogue Scale (VAS). The secondary endpoints included degree of cardiorespiratory steadiness and level of sedation measured by Ramsay sedation score. Satisfactions for patient and surgeon were measured via the satisfaction score.
PATIENTS AND METHODS
Patients’ recruitment
The study was conducted for 9 months started from February 2018 after ethics committee approval (Protocol ID: 180101). 30 patients diagnosed as AAA, were operated for EVAR and written informed high-risk consents for the anesthesia and operation were secured in this prospective study. The study was registered in Clinical Trials.gov ID: NCT03443518.
All patients were deeply assessed, through detailed history, physical examination, radiography of the chest, cardiac examination using electrocardiography (ECG), echocardiography, and laboratory testing. Duplex ultrasound for the aortoiliac, carotid, and lower limb arteries was done. Computed tomographic angiography of the entire abdominal and thoracic aorta was done also to assess the presence of any other aortic lesions and to decide the possibility of EVAR. Finally, all patients, were informed with clear language about both types of anesthesia. The patients were all given information about the risks and benefits of the EVAR procedure with the possibility for conversion to either open approach or GA.
Eligibility criteria: Elective patients diagnosed as AAA who will proceed to EVAR with exposure of the common femoral artery. Exclusion criteria: included emergency EVAR, hypertension (uncontrolled systolic arterial pressure ≥ 160?mmHg), diabetes mellitus (uncontrolled blood glucose ≥ 200?mg/dL), aneurysm of common femoral artery, patient receiving anticoagulant therapy, cerebrovascular disease and kidney disease (creatinine > 1.5?mg/dL).
Randomization was achieved using a computer-generated list and the sequence of randomization was done via sequentially numbered envelopes (SPSS program; SPSS Inc, Chicago, IL). A medical student was informed to prepare the infusion drugs. Another medical student who did not participate in induction of anesthesia but was only caring the patient intraoperatively, recorded the data and was not aware to the group type to avoid bias. On the other hand, the anesthesiologist concerned with the patient was aware to the group type (single blinded technique).
Anesthesia and monitoring
Prophylactic antibiotics (Cephazolin) were given to all patients intravenously. All patients were fasting for 8 hours. Premedication drugs were given in the form of midazolam 5 mg intramuscular and ondansetron 4 mg intravenously. After arrival of the patient, a bispectral index sensor (BIS) was put on the forehead of the patient and connected to an Aspect A2000 version monitor (Medical Aspect System, Inc. 141 Needham St. Newton, MA, USA). Pulse oximetry and 5-lead ECG were connected. A large bore venous cannula is mandatory if there is possibility for open surgery which could be associated with much blood loss. A 20-gauge radial arterial catheter was placed for continuous monitoring of blood pressure in the non-surgical access upper limb. Also, urine output was mandatory to be monitored. Simple oxygen face mask was applied at a rate of 6 L/min. A CO2 analyzer probe was put near the nostril of the patient for monitoring of end-tidal carbon dioxide.
Patients were divided into two groups with 15 patients each before starting the procedure. First group is the psoas compartment block (PCB group): 30 ml of bupivacaine 0.25 % infused over 3 minutes in addition to normal saline 0.9 % IV infused at the same rate of infusion of the remifentanil in the other group to ensure observer blindness.
In our study, we used a modified PCB technique which was used before by Mokini and his colleges (17) and it was done in lateral decubitus using stimulated needle (120 mm length) which was placed at the junction between the lateral one third and medial two-thirds of a straight line drawn at the interspace of L2–L3 in between the interspinous line and another line passing via the posterior superior iliac spine (PSIS), parallel to the interspinous line. If stimulation (twitching) of the anterior thigh was noticed, the needle was redirected cranially slightly. When the inguinal field twitching was achieved, bupivacaine 0.25 % 30 ml, was slowly injected over 3 minutes (Figure 1) (16).
Statistical methods
The obtained data were recorded and analyzed using the SPSS statistical package, version 22 (IBM Corp., Armonk, NY, USA). After performing tests of normality, student-t test and Mann-Whitney test were used to compare numerical data as appropriate, while c2 test was used to compare categorical data. The level of significance was considered at p-values less than 0.05.
Study populations
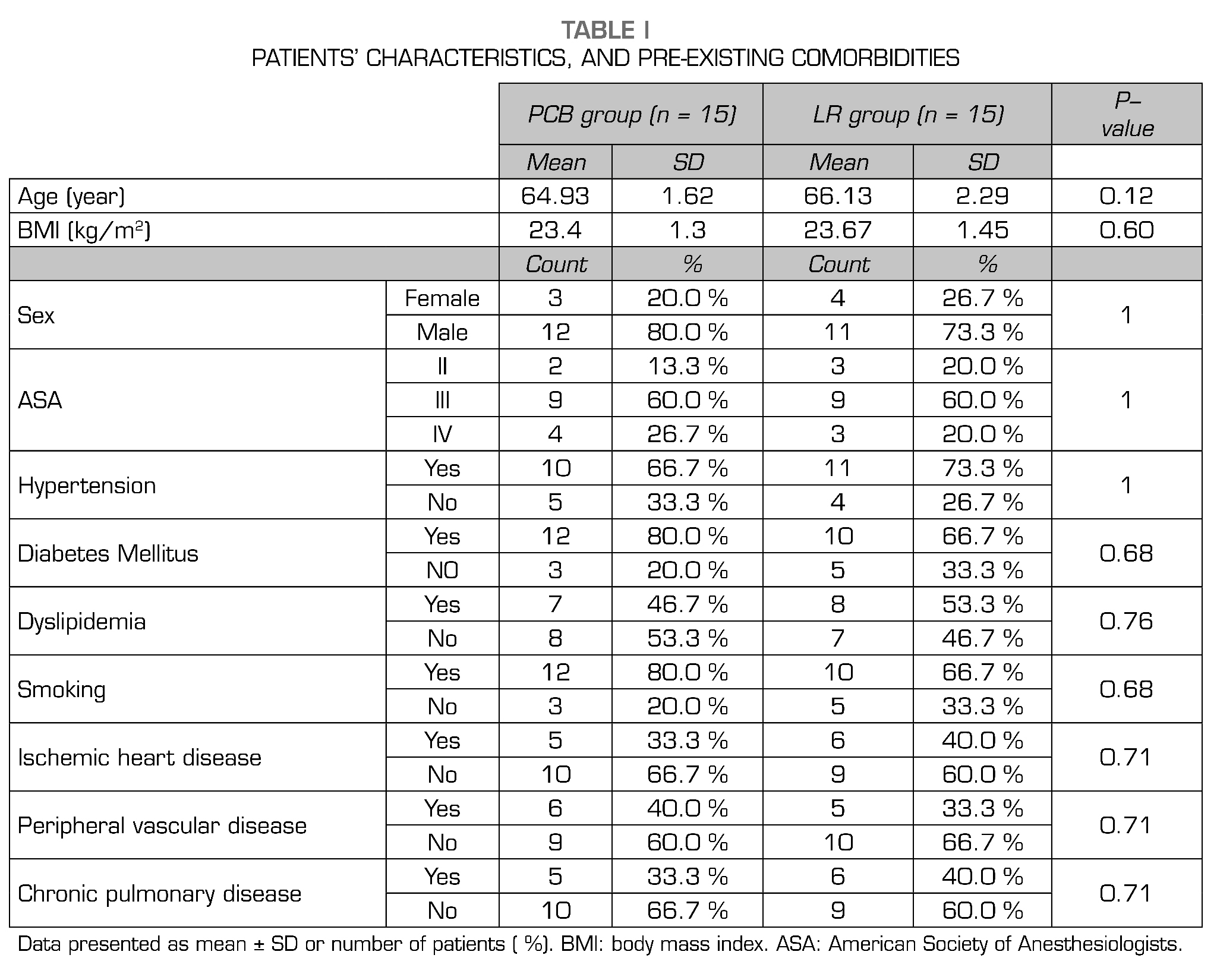
All patients completed the study with no conversion to general anesthesia. There were no significant differences between the groups concerning age, gender, ASA class and body mass index (BMI). Also, there were no statistical differences between both groups regarding the incidence of preexisting cardiac, pulmonary, or renal diseases (Table1).
Analysis of hemodynamic data
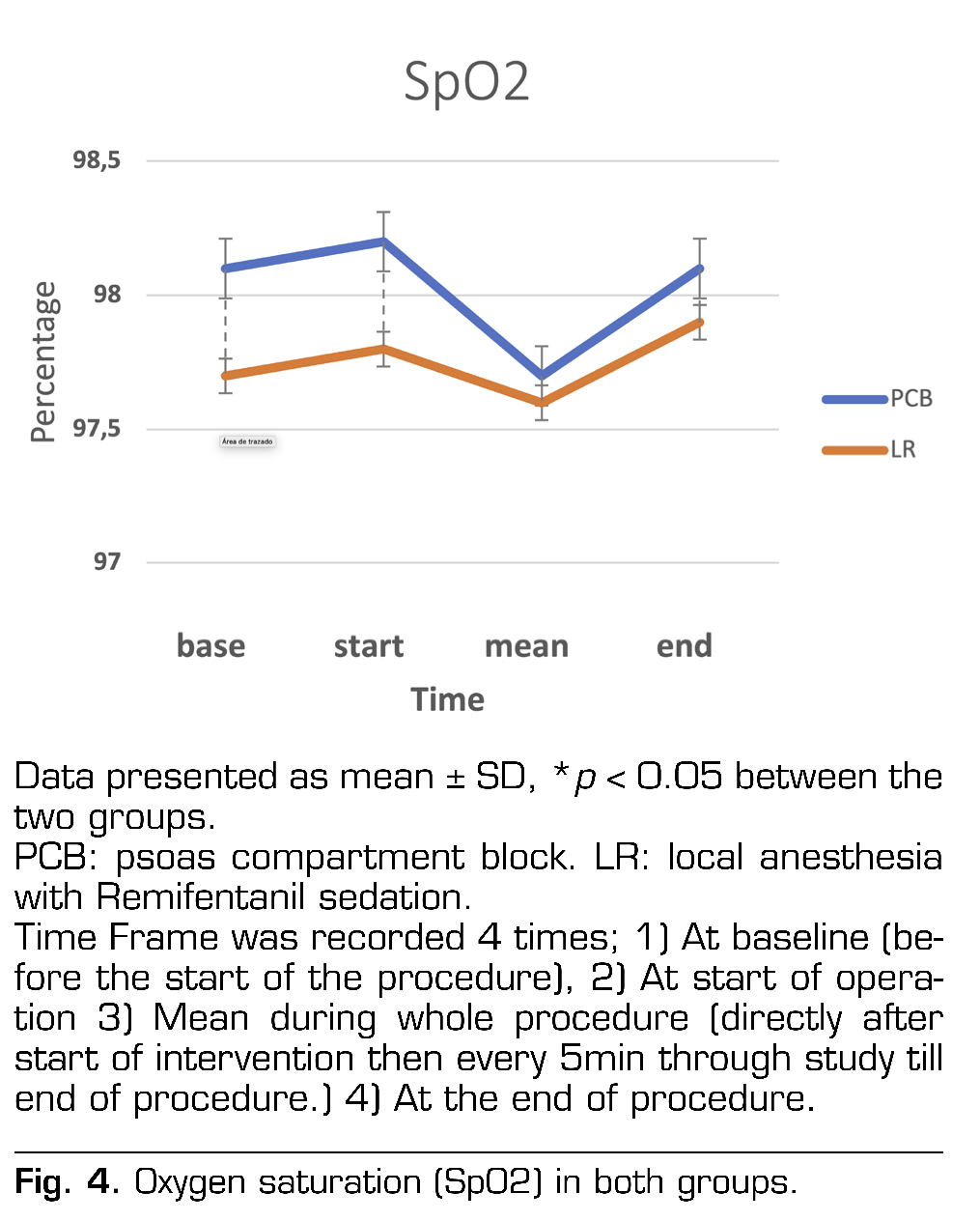
In patients under remifentanil sedation (LR group), the HR and MAP decreased significantly after induction of anesthesia and stayed significantly lower than PCB group throughout the procedure (p < 0.001) (Figure 2 and 3). As regard SpO2 data, it was comparable between both groups throughout the procedure (Figure 4). In the PCB group, 3 patients (20 %) received vasopressors and 2 patients (13.3 %) received vasodilators during the EVAR procedure. On the other group, sedation with remifentanil, 5 patients (33.3 %) needed vasopressors and 3 patients (20 %) needed vasodilators during the EVAR procedure. There was no statistically significant difference in the use of vasopressors and vasodilators between the two groups (p = 0.864).
Analysis of operative data
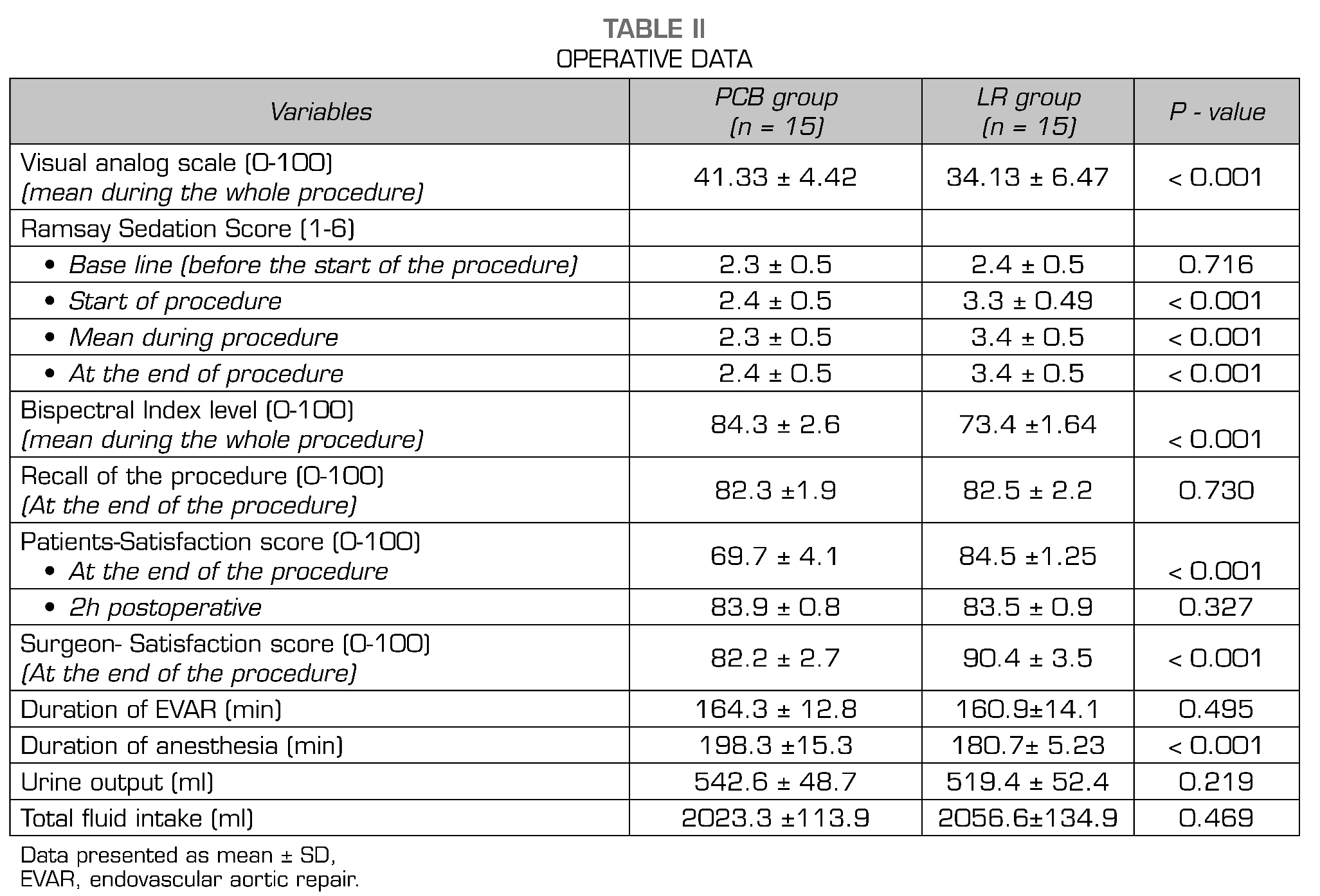
The mean VAS values showed statistically significant lower values in LR group when compared to PCB group (p < 0.001) (Table II). Ramsay Sedation score showed statistically significant deep sedation in LR group on comparison to PCB group (p < 0.001) (Table 2). Three patients developed agitation during the procedure in the PCB group and they received a small dose of midazolam to sedate them. Sedation with remifentanil was effective in all patients undergoing EVAR, allowing them to maintain satisfactory respiratory level and avoid desaturation. Also, BIS values were statistically lower in LR group than in PCB group (p < 0.001) (Table 2). All patients under sedation with remifentanil (LR group) did not complain about their general feeling, position, or pain intra- and postoperatively. So, their satisfaction scores were highly significant when compared to PCB group (p < 0.001) (Table 2). There was no statistical significance as regard recall of operative details between both groups (P = 0.730). Mean anesthesia time was significantly higher in PCB group (p < 0.001) (Table 2).
Clinical recovery data
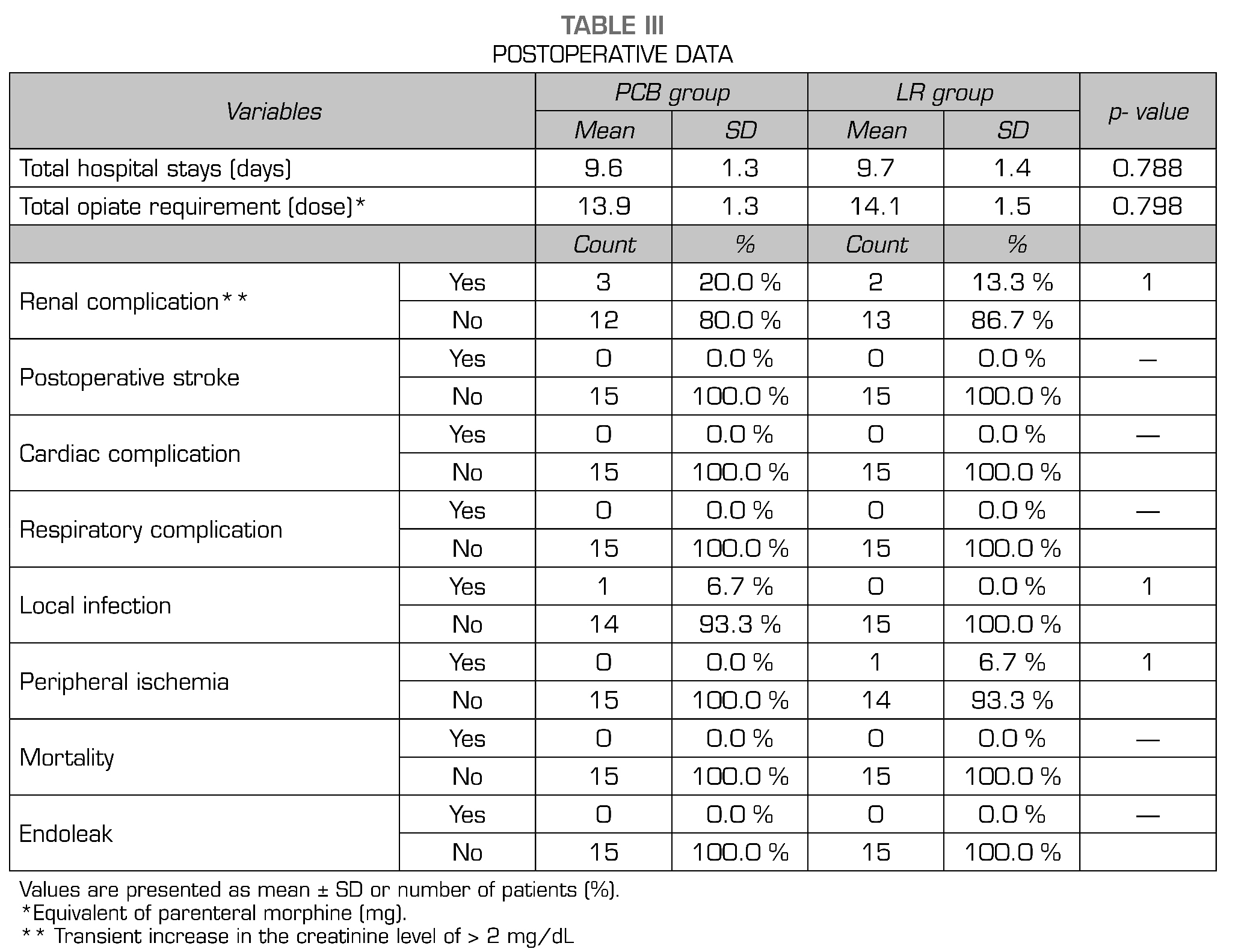
The incidences of cardiac, respiratory, renal, and neurologic complications also were not statistically different. Concerning total hospital stay, there were no statistically significant differences between both groups. There were no conversions to open repair or reoperation caused by migration of grafts or endoleak after EVAR in both groups (Table 3).
DISCUSSION
The current study demonstrated that EVAR under PCB or local anesthesia with Remifentanil sedation is safe and effective procedure for the treatment of aortic aneurysms. Remifentanil group provided significant lower values of VAS, HR, MAP than PCB group. Remifentanil group also achieved significant values of deep sedation without compromising respiration in comparison to PCB group. Also, patients in remifentanil group were significantly calmer and more cooperative with less BIS values than PCB group.
EVAR have a lot of benefits in high-risk patients, as this technique is less invasive than conventional surgery. It applies less hemodynamic changes result in faster recovery and less anesthetic and surgical complications (20). As the number of patients who undergo EVAR is growing up, tailored anesthetic considerations for EVAR are becoming increasingly essential.
Evidence based research did not confirm the best anesthetic choice for standard EVAR.
The literatures are restricted to descriptive, retrospective studies on patients undergoing infra-renal EVAR (21,22). To the best of our knowledge, this is the first prospective randomized study which evaluated the perioperative outcomes of EVAR performed under PCB or local anesthesia with remifentanil sedation.
The anesthetist usually decides the type of anesthesia according to multiple factors as the age of patient, nature of procedure and the preoperative medical condition (23).
Local Anesthesia is considered to be safe and good alternative for GA during EVAR (21). In a previous study (24), the regional anesthesia for EVAR decreased the duration of operation and postoperative ICU stay. Local Anesthesia also has provided the advantages of hemodynamic stability and is important in patients who have sever pulmonary disease (25). The previous results agreed with our study data, where local anesthesia and remifentanil sedation resulted in good recovery and hemodynamic stability.
Verhoeven and colleagues (7) proved less incidence of respiratory problems for local anesthesia compared with GA. In contrary to the previous study, de Virgilio and colleagues (27) reported comparable cardiac and respiratory complication rates in 229 EVAR procedures under GA versus local anesthesia. Different outcomes were noticed in another retrospective review for Henretta and his colleagues (26) who found that local anesthesia could not decrease cardiopulmonary mortality and morbidity rates in patients undergoing thoracic EVAR procedure.
Locoregional for the common femoral artery (CFA) cutdown provides a lot of advantages. It offers excellent analgesia intraoperative and for several hours later, decreasing the number of analgesic medications (28).
Henretta et al. (26) was the first one to describe the possibility of local anesthesia for EVAR in 1999, recording no deaths or significant morbidity in a group of 47 consecutive patients. These results were also agreed with Asakura et al. (24) who found that, local anesthesia usage was effective and accompanied by improvements in pulmonary morbidity and decreased ICU stay. In contrary to the previous study, Geisbusch et al (29) in his research, he gave local anesthesia in 183 EVAR patients, GA in 25 cases and RA in 9 cases. They found a 7.6 % GA conversion rate due to obstruction of the airway (29 %), persistent movement of the patient (7 %), anxiety (21 %), persistent coughing (21 %), patient discomfort (7 %) and emergency surgical conversion to GA (14 %). Fortunately, in our study, no single patient converted to GA may be attributed to good sedation and analgesia techniques.
Based on his experience, Mokini and his colleges (17) used the technique of modified access for PCB to approach awake inguinal surgery without any influence on hemodynamics. In our clinical study, PCB was associated with less hospital stay, less postoperative analgesic usage and minimal postoperative complications. However, PCB may be accompanied by complications like hypotension, systemic toxicity, subarachnoid or epidural spread, retroperitoneal hematoma and renal puncture (30,31). We do not consider PCB the only anesthetic technique for EVAR procedures, but in selected cases with difficult management, it represents a good alternative that deserves to be evaluated in larger randomized trials.
When we review our data comparing PCB or local anesthesia with remifentanil sedation, we found that in patients under remifentanil sedation, the HR and MAP decreased significantly after induction of anesthesia and stayed significantly lower than PCB group throughout the procedure (p < 0.001) which reflected clinically as in the PCB group, 3 patients (20 %) received vasopressors in comparison to sedation with remifentanil, 5 patients (33.3 %) received vasopressors during the EVAR procedure. But there was no statistically significant difference in the use of vasopressors between the two groups (p = 0.864).
Pain perception is considered the most important issue to differentiate between two experimental groups (32) which was found to be significantly less in intensity for the remifentanil group in comparison to PCB group (27.13 ± 6.47 vs. 41.33 ± 4.42, respectively, P < 0.001). Which proved that continuous infusion of remifentanil to be more effective than PCB in attenuating pain.
During monitored anesthesia care, a Ramsay score of 2-3 is considered good indicators of conscious sedation (33,34). Both groups had accepTable sedation levels all over the procedure inspite of the significant difference between both groups (PCB vs LA group) (2.27 ± 0.46 vs. 3.4 ± 0.5 with p < 0.001 respectively)
Another important indicator for any procedure under local anesthesia or sedation is satisfaction scores. All patients under remifentanil sedation (LR) group were cooperative and calm during EVAR. So, their satisfaction scores were highly significant in comparison to PCB group (P < 0.001).
Postoperatively, patients with EVAR require high dependency unit for continuous monitoring as regards blood pressure, blood gases, hemoglobin and coagulation parameters. The most important assessment is regular lower limb arterial examination. Usually, the pain is insignificance and could be treated with oral analgesics or minimal doses of opioids when needed (2). In our study, mean anesthesia time was significantly higher in PCB group in comparison to LR group (198.3 ± 15.3 vs. 180.7 ± 5.2, respectively, P < 0.001) which reflected clinically as total opiate requirement postoperatively was less in PCB group when compared to other group but without any statistically significance in between both groups (p = 0.798).
In another study, the group analysis under local anesthesia appeared to have shorter surgical times, shorter length of stay in the hospital and fewer postoperative complications in a review of 10 studies comparing regional to local anesthesia and involving 13,459 patients (21). However, our findings contradict the previous findings where there were no statistically significant differences between our two groups as regards total hospital stay which could be related to small number of patients in ours. The incidences of respiratory, neurological, cardiac and renal complications also were not statistically different.
Our investigation presents some limitations, which need to be considered. First, the anesthesiologist was aware by the mode of anesthesia. Moreover, this technique needs further study for the detection of the best site of injection and of the perfect local anesthetic volume for femoral artery exposure.
In conclusion, our findings high lightened the influence of both techniques using PCB or remifentanil with LA for conscious sedation and analgesia for patients with significant comorbidity during EVAR. They proved to be safe and effective in ASA III–IV patients undergoing EVAR. Also, both techniques provided sufficient cardiorespiratory steadiness, good sedation, and analgesia, resulting in an accepTable level of comfort for patients. However, remifentanil continuous infusion granted significantly more sTable pain control while maintaining similar levels of stability and analgesia of the currently used PCB.
ETICAL ASPECTS
The study was conducted after ethics committee approval (Protocol ID: 180101). Written informed high-risk consents for the anesthesia and operation were secured from all patients included in this prospective study. The study was registered in Clinical Trials.gov ID: NCT03443518.
FUNDING
This work was not supported financially by any grants from any private medical organization or our university.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
REFERENCES